When Children Who Stutter Present Co-Occuring Speech-Language Disorders: Some Clinical Considerations
 |
About the presenter: Dr. Kenneth J. Logan, CCC/SLP is a member of the Department of Communication Sciences and Disorders at the University of Florida, where he teaches, conducts research, and supervises clinical activities related to fluency disorders. He has presented many papers and authored a number of articles that deal with the nature and treatment of stuttering. |
When Children Who Stutter Present Co-occuring Speech-Language Disorders: Some Clinical Considerations
by Kenneth J. Logan
from Florida, USA
Stuttered speech is characterized by excessive or unusually long disfluencies or breaks in the flow of speech. Most often, the disfluencies include
(a) repetitions of words or parts of words,
(b) audible prolongations of consonant or vowel sounds, and
(c) inaudible prolongations or "blocks," in which speakers report being temporarily unable to initiate or move through speech sounds.
Most treatment approaches seek to help speakers modify speech-related behaviors in ways that reduce the occurrence of these disfluencies. With children, however, treatment sometimes is complicated by the presence of co-occurring speech-language disorders. The most common of these are language disorders and speech sound production disorders (i.e., articulation and phonology disorders). The purpose of this paper is to address five basic questions that arise when speech-language pathologists (SLPs) treat children who present stuttering plus articulation/phonology disorder (S+A/PD) or stuttering plus language disorder (S+LD). In doing so, we hope to provide readers with an overview of the salient clinical issues related to this segment of the clinical population.
Question 1: Is it unusual for children who stutter to have concomitant impairments?
Parents of children who stutter may ask whether it is common for other speech-language disorders to co-exist with stuttering. Results from some recent studies conducted with school-aged children who stutter offer some answers to this question. Arndt and Healey (2001) surveyed 241 SLPs from the United States. The SLPs provided data on 467 school-aged children who met their state's criteria for fluency impairment. According to the SLPs' reports, 14% of the children had phonological disorders, 15% had language disorders, and another 14% had phonological and language disorders. Thus, in all, 44% of the children who stutter had co-existing phonological and/or language disorders.
In a similar study, Blood, Ridenour, Qualls, and Hammer (2003) surveyed 1,184 American SLPs, who reported on the status of 2,628 children for whom they had documentation to support a diagnosis of stuttering and any of several other disorders. The SLPs reported that 63% of the children who stutter exhibited at least one co-existing speech, language, or non-speech-language disorder, and 44% exhibited two or more co-existing disorders. With regard to speech sound production, 34% of the children who stutter had concomitant articulation disorders and 13% had concomitant phonological disorders. With regard to language functioning, 6% of the children who stutter also had specific language impairment (SLI), and between 9% and 14% of the children also had impairments in receptive and/or expressive language that affected semantic, syntactic, and/or pragmatic functioning. The SLPs also indicated that, in the vast majority of cases, they considered the language and speech sound production disorders to be significant enough to treat.
In general, findings from the Arndt and Healey (2001) and Blood et al. (2003) studies are consistent with those from a host of previous studies (see Bloodstein, 1995 and Nippold, 1990, 2002 for reviews). Based on these findings, many researchers have concluded that language disorders and speech sound production disorders are more prevalent among children who stutter than they are among the general population. Nippold (2004, 2001) has argued that such a conclusion is premature. She contends that S+A/PD and S+LD children may simply be over-represented in the subject pools for these studies because they are more likely than children who present only stuttering (S-Only) to seek clinical services. Further research is needed to examine this possibility. Meanwhile, based upon current findings, it seems reasonable to conclude that impairments in language and speech sound production are fairly common among school-aged children who receive or qualify for fluency services. As suggested above, about 30% to 40% of these children who stutter can be expected to have co-existing impairments in language or speech sound production. In most cases, these impairments will be significant enough to warrant treatment.
Question 2: Are fluency disorders related to language or speech sound production disorders?
Because articulation, phonology, and language disorders co-exist with stuttering, some researchers have wondered whether the disorders are related. When considering questions about potential relationships among speech and language disorders, one first must remember that most children who stutter do not exhibit the various limitations that characterize articulation, phonology, and language disorders. Many children who stutter typically score within normal limits on tests of semantic and morphosyntactic development, and they seem to produce sentences and stories that generally are comparable in structure and complexity to those of children who do not stutter (Ratner, 1997). Those differences that have been detected tend to be subtle, and their significance is unclear. Thus, it seems unlikely that the neuro-developmental processes that give rise to phonemic substitutions, morphologic errors, sentence comprehension difficulties, and so forth, are necessary for one to stutter. It is conceivable; however, that the presence of such communicative difficulties could tax a weak speech production system in ways that make it more likely for speakers to repeat or prolong speech sounds. Indeed, recent research shows that children with expressive SLI produce more stutter-like disfluencies -- although not so many as to be considered "stutterers" -- than children with typical language skills (Boscolo, Ratner, & Rescorla, 2002; Hall 1999).
When considering potential relationships among speech and language disorders it also is important to consider how fluency, language, and articulation relate to one another in typical speech production. Fluent speech is the end product of a host of pre-linguistic, linguistic, and motoric events. In short, speakers must generate an intention to express, formulate linguistic codes that correspond to that intention, plan and execute a series of gestures that result in an acoustic representation of the linguistic codes, and monitor linguistic and articulatory outputs to ensure that the executed message matches the intended message. For speech to be fluent, a speaker must perform these tasks in an accurate, timely, and synchronized manner.
Of course, the speech production system does not always function this way -- even for non-stuttering speakers. Inaccuracies, delays, or asynchronies in linguistic processing sometimes occur, and when they do disfluent speech often results. Some linguistic formulation errors lead directly to speech disfluencies. For example, delays in lexical retrieval result in pauses, interjections, or word repetitions as the speaker attempts to access the desired information. Other types of linguistic formulation errors lead to speech disfluencies indirectly. For example, a speaker who says "green" when she intends to say "blue" may revise her message (i.e.., produce a type of disfluency) if she detects the error and elects to correct it. Some (e.g., Kolk & Postma, 1997) have hypothesized that the repetitions and prolongations that characterize stuttered speech are symptomatic of delays in phonological encoding. In this view, a speaker repeats or prolongs speech sounds until planning delays are resolved. While that remains to be seen, it seems evident that children who have difficulty with one or more component of the speech production process will be at greater risk for producing speech disfluencies (although not necessarily stutter-like disfluencies) than children who do not have such difficulties.
Although most children who stutter seem to perform comparably to nonstuttering children on common clinical measures of linguistic competence, results from recent research suggest that they do not fare as well on comparisons that look at processing speed. Numerous studies have found that children who stutter take longer than their nonstuttering counterparts to initiate simple speech- and non-speech-based responses to stimuli (Logan, 2003). Children who stutter also seem to take longer than nonstuttering individuals to plan syntactic information (Anderson and Conture, 2004). So, while stuttering does not appear to be an "articulation disorder" or a "language disorder" in the classic sense of these terms, there is growing evidence that children and adults who stutter have difficulty executing language-related tasks, particularly difficult or demanding ones, as efficiently as people who do not stutter.
Question 3: Does the presence of a concomitant disorder affect stuttering severity?
Some parents may wonder if the presence of co-existing articulation or language disorders will make their child's stuttering worse or different in character than it otherwise might be. Unfortunately, there is little or no research on how the fluency skills of S+LD and S-Only children compare. At least one study has compared the fluency skills of S-Only children with those of children with stuttering and disordered phonology, however.
Wolk, Edwards, & Conture (1993) reported no significant differences between children with stuttering and disordered phonology (S+DP) and S-Only children in stuttering frequency, duration, or severity. However, children in the S+DP group did produce significantly more sound prolongations (37% of total disfluencies) than children in the S+NP group did (19% of total disfluencies). Children in the S+DP group were also compared to a group of children with normal fluency and disordered phonology (DP-Only). Statistical analysis showed no significant differences between the groups in terms of phonetic inventory, percent of consonants correct, number of phonological processes per word, and frequency of occurrence for 15 phonological processes. Overall, the findings from this study do not provide strong support for the idea that the fluency and phonology skills of S+DP children differ markedly from those of S-Only and DP-Only children. Further research is needed, however, to examine the effect that the severity of a disorder has upon these relationships.
Question 4: Should the disorders be treated separately?
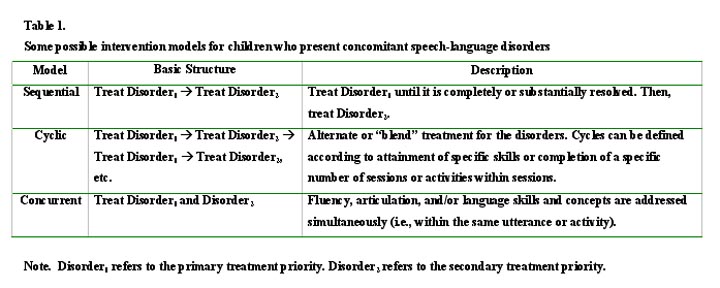
Clinicians may find it difficult to determine how to structure a treatment program for S+A/PD and S+LD children. Three general treatment models have been discussed in the literature. These are outlined in Table 1. To our knowledge, there has been no research to date to examine whether one treatment model is more effective than another. Clearly, this is another area where research is needed.
Determining which model is most appropriate for a particular child depends, in part, upon whether one disorder is considered a higher priority than another. SLPs can rank treatment priorities by considering
(a) the extent to which a disorder affects the child's performance and participation in daily activities,
(b) the child's ability to monitor or alter multiple communicative behaviors simultaneously, and
(c) the likelihood that a disorder will remit without treatment (Logan & LaSalle, 2003).
Generally, the sequential model seems best suited for cases in which one disorders has relatively little impact upon a child's daily functioning or when at least one of the disorders shows signs of remitting (e.g., there is evidence of emerging skills or structures). Usually, both disorders will affect performance, so the sequential approach carries the risk of complicating treatment for whichever disorder is not treated first. In contrast, a cyclic model seems best suited for cases where two or more disorders have a substantial negative impact upon communicative functioning. The cyclic model requires children to focus primarily on only one disorder per activity. As such, it seems particularly applicable for the beginning stages of treatment, when children are establishing basic skills.
The concurrent model, which entails simultaneous management of two or more disorders, can place varying demands upon children, depending upon the type of activity being done. Thus, the model seems appropriate to use at any stage of therapy, provided the SLP attends carefully to task demands. For example, an activity that requires an S+LD child to incorporate interrogative reversal on all questions while simultaneously applying easy onsets at the start of each breath group during conversation would be relatively difficult, and most appropriate for use during the later stages of therapy. Alternately, an activity that requires an S+A/PD child to judge whether paired words produced by the SLP are the same and then respond "yes" or "no" while using easy onset would be relatively easy, and appropriate for any stage of therapy.
Of course, SLPs are not bound to one model for the duration of treatment. Rather, a clinician might initially address a child's disorders in a cyclic manner, and then shift toward a concurrent model after the child has firmly established fundamental skills and is ready to generalize them to out-of-clinic contexts.
Question 5: What can be expected with regard to treatment outcomes?
Many parents are interested in knowing how much their child's communication skills can be expected to improve and how long it will take their child to improve them. Such questions are difficult to answer precisely because, to date, the subject of treatment outcomes with S+A/PD and S+LD children has not been well researched. In recent years, there have been calls for so-called frontline clinicians to get involved in clinical research. S+A/PD and S+LD children would be excellent groups for clinicians to investigate, as there are many very basic research questions waiting to be answered through single-subject or group designs. In the absence of treatment outcome data, an obvious strategy would be to implement interventions that have been demonstrated to be effective with the respective disorders. These "proven" interventions could then be delivered within the broader context of the three treatment models described above. Because data on treatment efficacy are still emerging, even this is not as straightforward as it sounds.
Research has repeatedly shown that fluency, articulation, and language skills are interrelated. For instance, the syntactic complexity of a sentence affects how fluently children speak and how accurately they produce consonants. So, regardless of which intervention approach is selected, SLPs need to have a keen sense of how difficult a particular articulation, fluency, or language target is. Many clinicians (e.g., Conture, Louko, & Edwards, 1993; Ryan & Van Kirk, 1974) have stressed the importance of introducing fluency skills in either "low demand" contexts (e.g., isolated words, short phrases) or with language forms that are well mastered, and then systematically extend the skills to other contexts by gradually increasing utterance length and complexity. Task complexity can be managed in other ways, however. For instance, receptive tasks (e.g., judging whether a particular word contains a target phoneme, judging whether a clinician's sentence is grammatical, judging whether a clinician's sentence contains word repetitions) are usually easier than expressive tasks. Because speech fluency can be affected by articulatory and linguistic demands, SLPs and parents should also be aware that treatment activities have the potential to temporarily exacerbate a child's stuttering. As Ratner (1995) succinctly put it, "Efforts to remediate areas of deficiency are likely to exacerbate patterns of fluency failure."
Finally, children with multiple impairments usually have a wide assortment of skills that need to be developed. Because of this, SLPs, parents, and other adults must be particularly careful to evaluate performance during any particular therapy activity in relation to the specific objective for that activity. For example, if an activity is designed to target phonological skills, then fluency "errors" should generally be ignored. Similarly, if an activity is designed to target fluency skills, then phonological errors should generally be ignored. As children develop the competence to manage fluency, articulation, and language concerns concurrently, expectations can be increased. Until such a time, however, the general rule in any clinic should be "no piling on!"
Concluding remarks
In this paper, we have raised five fundamental questions that pertain to the clinical management of children who present stuttering and co-existing language and speech sound production disorders. As can be seen, some of the questions can be answered with a fair degree of specificity, while others are nowhere near being settled! With additional research, we can surely gain a better understanding of issues related to the nature and treatment of S+A/PD and S+LD children. Clinicians are well-positioned to participate in this research effort, particularly in matters related to treatment outcomes.
References
Arndt, J. & Healey, E.C. (2001). Concomitant disorders in school-aged children who stutter. Language, Speech, and Hearing Services in Schools, 32, 68-78.
Blood, G.W., Ridenour, Jr., V.J., Qualls, C.D., & Hammer, C.S. (2003). Co-occurring disorders in children who stutter. Journal of Communication Disorders, 36, 427-448.
Bloodstein, O. (1995). A handbook on stuttering. (5th Ed.). San Diego: Singular Publishing Group, Inc.
Boscolo, B., Ratner, N.B., & Rescorla, L. (2002). Fluency of school-aged children with a history of specific expressive language impairment: An exploratory study. American Journal of Speech-Language Pathology, 11, 41-49.
Conture, E.G., Louko, L.J., & Edwards, M.L. (1993). Simultaneously treating stuttering and disordered phonology in children: Experimental treatment, preliminary findings. American Journal of Speech-Language Pathology, 2, 72-81
Hall, N.E. (1999). Speech disruptions in pre-school children with specific language impairment and phonological impairment. Clinical Linguistics and Phonetics, 13, 295-307.
Kolk, H., & Postma, A. (1997). Stuttering as a covert repair phenomenon. In R.F. Curlee & G.M. Siegel (Eds.), Nature and Treatment of Stuttering: New Directions, 2nd edition (pp.182-203). Boston: Allyn & Bacon
Logan, K.J. (2003). The effect of syntactic structure upon speech initiation times of stuttering and nonstuttering speakers. Journal of Fluency Disorders, 28, 17-36.
Logan, K.J. & LaSalle, L.R. (2003). Developing intervention programs for children with stuttering and concomitant impairments. Seminars in Speech and Language, 24(1), 13-19.
Nippold, M.A. (2004). Phonological and language disorders in children who stutter: Impact on treatment recommendations. Clinical Linguistics and Phonetics, 18, 145-160.
Nippold, M.A. (2002). Stuttering and phonology: Is there an interaction? American Journal of Speech-Language Pathology, 11, 99-110.
Nippold, M.A. (2001). Phonological disorders and stuttering in children: What is the frequency of co-occurrence? Clinical Linguistics and Phonetics, 15, 219-228.
Nippold, M.A. (1990). Concomitant speech and language disorders in stuttering children: A critique of the literature. Journal of Speech and Hearing Disorders, 55, 51-60.
Ratner, N.B. (1997). Stuttering: A psycholinguistic perspective. In R. Curlee & G. Siegel (Eds.), Nature and treatment of stuttering: New directions (2nd ed., pp. 97-127). Boston: Allyn & Bacon.
Ratner, N.B. (1995). Treating the child who stutters with concomitant language or phonological impairment. Language, Speech, and Hearing Services in Schools, 26, 180-186.
Ryan, B.P., & Van Kirk, B. (1974). The establishment, transfer, and maintenance of fluent speech in 50 stutterers using delayed auditory feedback and operant procedures. Journal of Speech and Hearing Disorders, 39, 3-10.
Wolk, L., Edwards, M.L, & Conture, E.G. (1993). Co-existence of stuttering and disordered phonology in young children. Journal of Speech, Language, and Hearing Research,36, 906-917.
September 7, 2004
After the conference is over, you may address correspondence to:
Kenneth J. Logan, Ph.D.
Department of Communication Sciences and Disorders
343 Dauer Hall
University of Florida
Gainesville, FL 32611-7420
logan@csd.ufl.edu