Providing Help for People Who Stutter: A World View
 |
About the presenter: Kenneth (Ken) St. Louis, Ph.D., CCC-SLP, (West Virginia University, Morgantown, West Virginia), has worked in the area of stuttering and cluttering for his entire career of more than 30 years. He has essentially recovered from a stuttering problem that began in early childhood and persisted into his early adult years. St. Louis considers himself eclectic in views about the nature and treatment of stuttering, having developed programs of research into such areas as: measuring public attitudes toward stuttering, identifying communication disorders that coexist with stuttering, exploring the relationship between linguistic and motoric aspects of stuttering, and defining cluttering. |
This paper is also available in PDF format for anyone who wishes to print it out. The graphics will be clearer in PDF format.
Providing Help For People Who Stutter: A World View
by Kenneth O. St. Louis
from West Virginia, USA
Adapted from a lecture delivered to faculty, students, self-help representatives, and guests at Southwestern University "Neofit Rilski" in Blagoevgrad, Bulgaria on May 26, 2004 on the occasion of the author receiving an honorary doctorate (Doctor Honoris Causa) from the University.
The lecture and follow-up questions were translated orally into Bulgarian by Dr. Dobrinka Georgieva, Vice Dean of the Faculty of Philosophy and Chairperson of the Department of Logopedics. The topic was of particular interest to this audience, given the desire of Bulgaria, a former Soviet Bloc country, to define logopedics (i.e., speech-language pathology) as a discipline separate from special education.
This paper summarizes some thoughts about the development of channels, methods, and infrastructure for helping people who stutter around the world. As most people visiting this on-line conference are aware, there are countries where it is very common for stutterers to receive therapy from trained professionals. There are also countries where very little if any professional help is available. Obviously, there are countries between these two extremes where there are growing and changing treatment infrastructures for those who stutter.
The following analysis could be viewed from an historical perspective in the modern treatment of stuttering, as in North America (e.g, Bloodstein, 1995; St. Louis, 2003), but is also about what is or could be happening in various countries around the world today. Although these ideas pertain to stuttering, they are relevant to any of the speech, language, or hearing disorders.
I have constructed a figure that provides an overview of my thoughts about development. It will be described one component at a time.
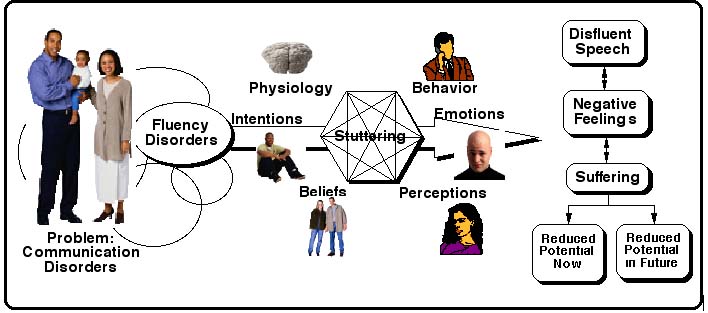
The first graphic shows that there are a number of communication disorders, and one group of them is called "fluency disorders." Stuttering is the most common of these fluency disorders and afflicts about 5% of people sometime in their life. Many simply "grow out of it," leaving about 1% of adults with chronic stuttering. I have borrowed John Harrison's "Stuttering Hexagon" (Harrison, 2004, May 5) to illustrate. It shows that stuttering involves at least six interrelated components: physiology (including genetics), behavior (including the stuttering itself), emotions, perceptions, beliefs, and intentions. Disfluent or stuttered speech, negative feelings (e.g., fear and embarrassment), and suffering combine to manifest in not reaching one's full potential either now or in the future (St. Louis, 2001).
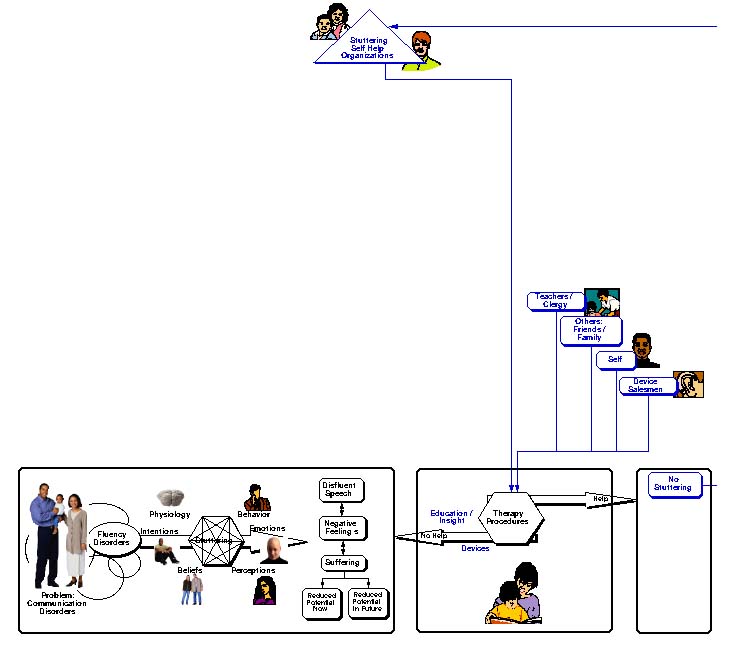
Stuttering, like all other communication disorders, is a societal problem. We are concerned about stutterers not because they will die without treatment but because we do not want them to suffer needlessly. In any society, before there is a professional group whose job it is to try to help those who stutter, there are a few groups that try to help as seen in the second graphic. These are caring people who possess the intuitive personal skills that allow them to help others who are troubled. This group includes teachers, religious leaders, family members, and friends who want to help. Let me also mention that there is a new and growing group of entrepreneurs who market electronic devices, such as miniaturized altered auditory feedback devices that look like hearing aids, directly to people who stutter. Taken together, typical goals of these efforts are either to help stutterers understand their problems or to stop stuttering altogether. (I should point out that a substantial percentage of stutterers do not receive the help they expect from electronic devices alone, bu the effectiveness can be improved by concomitant speech therapy.) Finally, the graphic shows the stuttering self-help movement that has grown out of people who have often learned to help themselves and therefore want to help others. I'll mention more about these individuals later.
With these efforts, some stutterers improve, but many do not. More important, most stutterers in developing countries "and many even in the most developed countries" are not aware that any help is available to them at all. For this reason, citizens, usually through volunteer civic groups, decide that something systematic must be done to help those who stutter or who will stutter. The thicker lines in the next graphic indicate these powerful influences.
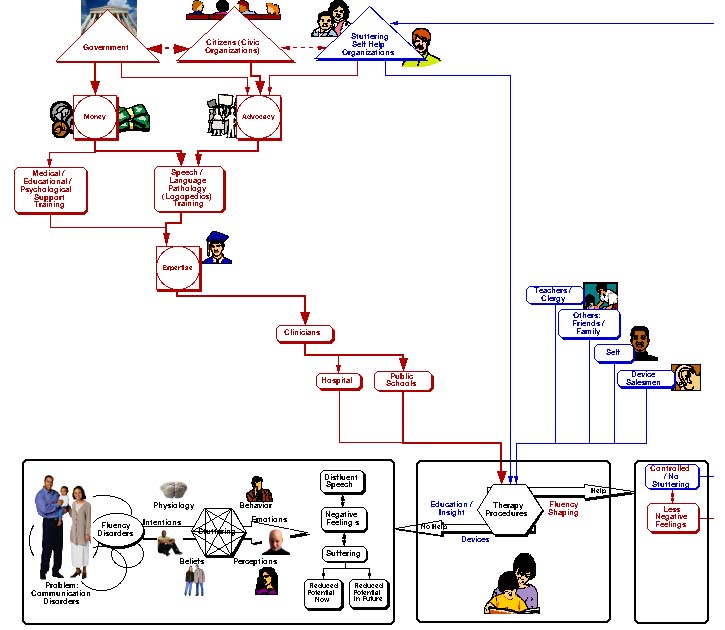
To inaugurate any new discipline requires at least three important components: (1) advocacy, (2) money, and (3) expertise. It begins with advocacy, primarily by civic groups. Until recently there has been no organized stuttering self-help movement, but in the past decade, this has changed. Now, self-help groups have become important advocacy influences, especially in countries with no therapeutic infrastructures. Advocates increasingly interact with government leaders. Eventually, money is appropriated, and training programs are instituted to create a cadre of trained professionals.
Typically, the first step is to develop new departments for speech-language pathology "or logopedics" that partner with existing departments, perhaps special education, psychology, or various medical fields in universities. The new speech-language pathology departments then set about to train clinicians to treat stuttering and other communication disorders. Often, jobs for new clinicians are located within the country's school system primarily because the mechanisms for gaining access to those with problems is probably easiest through the existing education system. For this reason, many training programs become part of education or special education, which I submit is often not the best fit. (See comments below.) Sometimes the first generation of clinicians are placed in hospitals. In any case, trained clinicians often work with stutterers and, in addition to the aforementioned goals, seek to help them speak more fluently and, with practice, to experience less fear and avoidance of speaking.
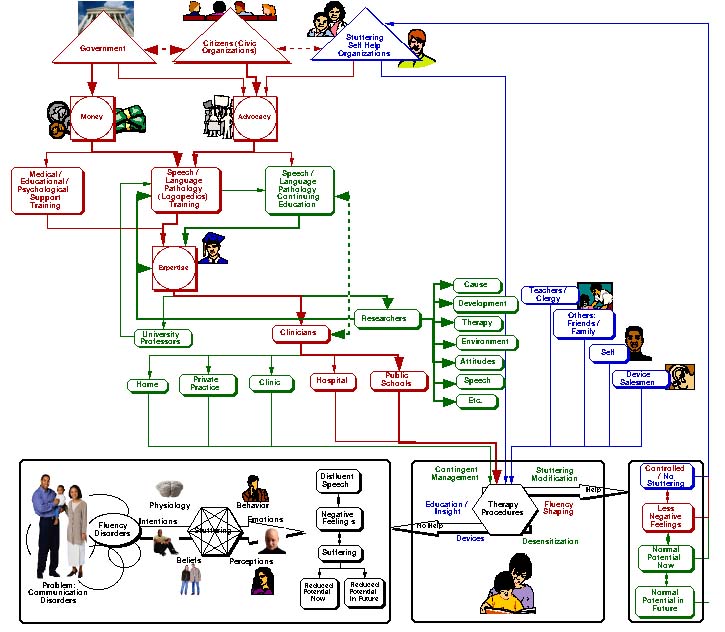
So far, I have summarized the first important phase in developing an infrastructure for treating communication disorders. However, after some years, it typically becomes evident that therapy is often not as effective as anticipated, that some of the information taught in the training programs may not be relevant to the day-to-day problems that clinicians encounter, that much more new information is required, and so on. This is the beginning of a long process of maturing and expanding of the field. In the third graphic, green lines summarize some of those developments that we have experienced in the USA and that are currently occurring in other countries, such as Bulgaria.
Probably the most important addition to the system is research. Researchers at universities or government agencies are trained and carry out research focused on the entire range of questions regarding the disorders and their treatment. For stuttering, the search for a cause has recently shifted to better understanding of genetics and the brain function. But research also focuses on the environment, emotions, and other aspects of the disorder. For example, research has revealed that stuttering manifests differently in children and adults. Researchers also look at therapy strategies, the outcome of therapy, and the long-term maintenance of improvement. There are literally thousands of questions that are addressed by researchers, and the emerging answers feed back into the training programs and growing body of knowledge or expertise.
Other influences are important as well. University professors are trained to teach at new training programs. Nevertheless, clinicians remain the main focus of training programs and public schools and hospitals are still important. In the USA, it is clear that the problem of stuttering cannot be adequately addressed only in the schools by those trained as special educators. Two- and three-year-old children who stutter are often best treated in clinics, private practices, or even in their own homes. Adults who stutter typically cannot be addressed in schools or hospital settings. Moreover, specialized training is necessary in other disorders, such as aphasia, to prepare clinicians to work in institutions for the growing elderly populations in the world. For stuttering and many other disorders, the education or special education model often cannot adequately train clinicians to function in all of the relevant settings. On the other hand, training in purely medical settings often does not prepare students for their school experiences. This is why, in my opinion, some of our best training programs are located in colleges of Allied Health, along with physical and occupational therapy, nursing, social work, and even epidemiology.
As we have come to better understand the clinical process, we have learned that we must individualize our therapies for specific stutterers. We often teach them to modify their stuttering into an easier form of stuttering"rather than trying not to stutter" and accompany this with considerable effort on learning to manage their fears. Sometimes we combine stuttering modification with fluency shaping. Sometimes we focus almost exclusively on learning not to avoid stuttering. Therapy in the USA is now being regarded more and more from the perspective of "efficacy" (i.e., "Is it effective?"). Insurance companies are beginning to ask such questions before paying for therapy. In order to determine whether or not therapy is effective, we are being forced to develop new instruments that measure the extent to which one's actual life has been improved as a result of therapy. For example, does a person after therapy use the telephone more" or more effectively" at work than he did before therapy?
It has become clear that professionals are never adequately trained for their entire careers. As everyone knows, the information age is here, and new information will replace current information in a few years. It is important to provide a wide variety of strategies for trained clinicians and others to update their training with relevant information throughout their careers. In the USA, we have inaugurated a new program to recognize speech-language pathology specialists who treat stutterers and to develop mechanisms for maintaining their "specialty recognition." Additionally, many clinicians from the USA and abroad have attended workshops sponsored by the Stuttering Foundation of America and National Stuttering Association designed to provide continuing education to clinicians.
What does the future hold? I do not pretend to know the answers, but let me make some observations and guesses. As I mentioned, there is growing collaboration among researchers, clinicians, and people who stutter around the world. As shown in the last graphic, information flows into and out of every country and affects the entire system. The dotted lines reflect influences both ways. The added pink lines show that influences from other countries affect the self-help movement and other advocacy organizations. For example, national self-help associations speak for stutterers all over their various countries. Most European associations are members of the European League of Stuttering Associations (ELSA), and most national association are members of International Stuttering Association (ISA). International connections are also established and strengthened through interactions on this annual International Stuttering Awareness Day on-line conference every October.
International collaborations carried out by scientists and clinicians affect the expertise brought to fluency disorders through published articles, chapters, and books; training programs; continuing education; and advocacy and support from international community organizations.
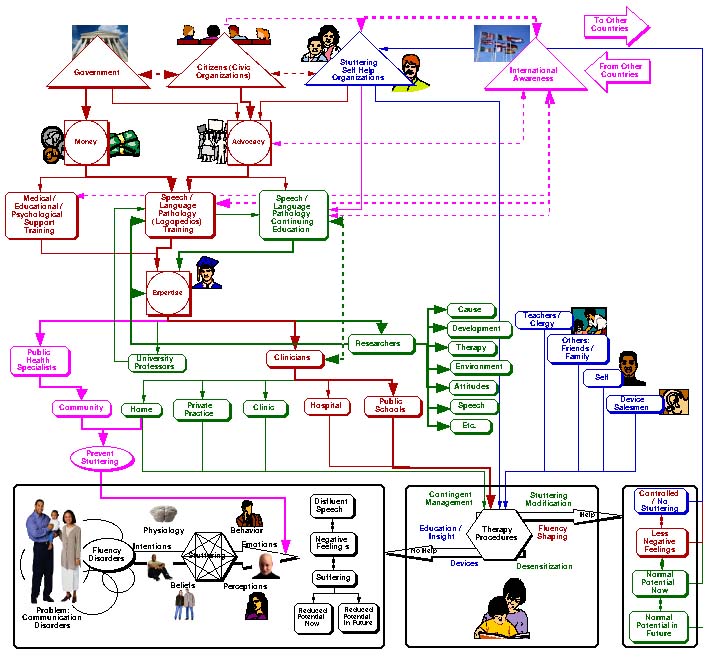
This figure is completed with the highlighting of one area that I suspect will emerge in the area of stuttering. This is the area of prevention that has begun to be recognized in the USA as an important and viable enterprise. Though not yet present, I forsee a new group of specialists whom I refer to as "public health specialists" on the chart. Their actual titles could vary considerably. These individuals will work with communities and individuals in their homes, along with appropriate school and medical personnel, to prevent the occurrence of stuttering in the first place. We know, for example, that if we can intervene very early in stuttering, children often grow up never remembering that they stuttered at all. As the roles of genetics and brain function begin to become better understood, there may well be drugs that will be developed that, combined with early intervention, might help at-risk children never to start stuttering at all.
I cannot predict the future, but there is no doubt that in the field of stuttering, as in all the communication disorders, changes will occur. It is likely that more and more developing countries will adapt infrastructures similar to those outlined here in order to meet the needs of their stuttering populations seeking help. It is also likely that new models and methods of treatment will emerge, which in turn will affect existing infrastructures.
References
Bloodstein, O. (1995). A handbook on stuttering, 5th ed. San Diego, CA: Singular.
Harrison, J. C. (2004, May 5). Developing a new paradigm for stuttering. The National Stuttering Association. Website visited 5/5/04. http://www.mnsu.edu/comdis/kuster/Infostuttering/Harrison/hexagonarticle.html
St. Louis, K. O. (2001). Living with stuttering: Stories, basics, resources, and hope. Morgantown, WV: Populore.
St. Louis, K. O. (2003). In the USA, can the field of fluency disorders recover? Pró-Fono Revista de Atualização Científica, , 15, 105-109.
June 14, 2004