What We Know About Neurogenic Stuttering - Etiology, Diagnosis and Treatment Strategies
 |
About the presenter: Kathrin Koenig, PhD, SLP, is a therapist, speaker, and lecturer in the area of fluency disorders. After completing her academic studies in speech-language pathology and rehabilitation science at the University of Dortmund, Germany, she started working at a private institution for speech and hearing science, where she specialized in treating people who stutter. After completing research on neurogenic stuttering treatment, she obtained her doctorate from the University of Dortmund. Apart from neurogenic stuttering, her research interests include idiopathic/developmental stuttering, evidence-based treatment, and childhood language. |
What we know about neurogenic stuttering - etiology, diagnosis and treatment strategies
by Kathrin Koenig
from Germany
Van Riper describes stuttering as "a complicated, multidimensioned jigsaw puzzle, with many pieces still missing" (Van Riper, 1982, 1). We can think of a puzzle that can be completed gradually by the more research we do. The image of a puzzle matches very well not only developmental stuttering but also the kind of stuttering, this paper deals with: neurogenic stuttering.
Neurogenic stuttering occurs more rarely than developmental stuttering does. It appears like a complicated puzzle consisting of many different pieces that can be put together and a whole bunch of other pieces we still have to find and add to the multidimensioned structure.
Turning to those pieces of the puzzle that can already be put together -- What do we know about this speech disorder which is called "neurogenic stuttering"? We will try to look behind the surface and see what the term "neurogenic stuttering" implies.
We can approach the term by breaking it up into its two pieces "neurogenic" and "stuttering".
"Stuttering" has been defined numerously. A huge variety of definitions has been put forth in international literature, however no one of those has overall acceptance. But we can still summarize that stuttering is a disorder of fluency. It implies disruptions in the production of speech sounds by the so called "core symptoms" which are repetitions, blocks and/or prolongations.
"Neurogenic" characterizes the neurological background, some kind of neurological disorder or disturbance that precedes or accompanies the onset of those repetitions, blocks and/or prolongations.
Up to this point, we can state that the term neurogenic stuttering is used as a description of stuttering symptoms that occur in association with a neurological disorder or disturbance.
But what about those other terms we come across in international literature? Dealing with those neurologically associated stuttering symptoms we do not only read about "neurogenic stuttering" (e.g. Baumgartner & Duffy,1997; Curlee, 1995, Helm, Butler & Canter, 1980, Koenig, 2009) but also about "dysfluency" in general (Horner & Massey, 1983; Janati, 1986) "dysfluent speech" (Yairi, Gintautas & Avent, 1981), "repetitive verbal behavior" (Christman, Boutsen & Buckingham, 2004), "speech difficulties resembling stuttering" (Lebrun, Devreux & Rousseau,1986), "organic stuttering" (Van Riper, 1982) "acquired stuttering" (e.g. Market et al., 1990; Marshall & Neuberger, 1987; Ciabarra et al., 2000), "thalamic stuttering" (Van Borsel, Van Der Made & Santens, 2003), "dysarthric stuttering, apraxic stuttering, dysnomic stuttering " (Canter, 1971), and "cortical stuttering" (e.g. Rao, 1991; Rosenbek et al., 1978; Horner & Massey, 1983).
So what do these terms stand for? Can they all be used for one and the same speech disorder?
"There is no general agreement about what dysfluencies that begin in adulthood should be called. This perhaps reflects uncertainty about their relationship to developmental stuttering, limited understanding of what the dysfluencies actually reflect, and the considerable heterogeneity in their character, etiology, physiology, and localization" (Baumgartner & Duffy, 1997, 75).
However, I prefer the term "neurogenic stuttering" which characterises both the symptomatology, and the neurological causation.
The complexity of neurogenic stuttering is not only reflected in the various labeling but also in the large number of definitions that can be found in international literature. Just as developmental stuttering, neurogenic stuttering has not been defined universally.
In order to provide a unique understanding of neurogenic stuttering in this article, we will try to define neurogenic stuttering on the basis of literature, referring to different authors. According to Van Borsel et al. (1997), Grant et al. (1999), Leder (1996) and Helm-Estabrooks (1986) we can speak of neurogenic stuttering if a person develops sound or syllable repetitions, prolongations or blocks in direct correlation with an underlying neurological disorder or disturbance. The stuttering symptoms can occur for the first time in life. It is also possible that existent idiopathic stuttering symptoms considerably change or worsen. Basically, the appearance of neurogenic stuttering is possible at any age. But, with regard to the indispensable neurological background, in the majority of cases the onset lies in adulthood. The presence of a neurological background is considered a prerequisite for neurogenic stuttering. Even though neurogenic stuttering occurs most often in adults, due to the preceding neurological disorder or disturbance, it is not impossible for children to acquired neurogenic stuttering as well, after some kind of neurological event.
So what kind of neurological disorder or disturbance can be associated with neurogenic stuttering?
There is no reliable taxonomy. Neurogenic stuttering is known to possibly occur in association with any kind of neurological disturbance. It has been observed with a huge variety of neurological diseases or injuries including: Cerebrovascular disease, head trauma/ traumatic brain injury, neurodegenerative disease, tumor, epilepsy, intoxication, neurosurgery and other diseases of the central nervous system such as dementia, migraine attacks and so forth.
"The question remains as to what sequence of events, or combination of features, is necessary to produce a form of stuttering in some adults" (Helm, Butler & Canter, 1980, 278).
Also, the question remains: Why do some people with neurological disorders start to stutter while others don't?
Even though, these questions have already been posed decades ago, we are still not able to find an adequate answer to those yet. "Why some cortical lesions result in cortical stuttering and others do not [...] remains unclear" (Horner & Massey, 1983, 75). We can conclude that more intensive and systematical research is needed to better understand the pathomechanism of neurogenic stuttering with regard to both the causal factors and the upholding factors.
Turning to the diagnostic process -- How do we recognize neurogenic stuttering? Which symptoms typically characterize neurogenic stuttering? Are there any similarities all neurogenic stuttering individuals have in common?
The ICF, the international classification of functioning, disability and health, - a classification system which was developed by the Word Health Organization -- can be used as the basis for both the diagnostic and the therapy process. The ICF focusses not only on the body functions, the stuttering moments, but also and particularly on the individual's activities and participation as well as on the personal factors (e.g. stress, frustration, shame) and the environmental factors (e.g. familial support, availability of adequate treatment and so forth).
Consequently not only is speech fluency tested but also the presence of other speech problems such as aphasia, apraxia of speech or dysarthria that may accompany neurogenic stuttering (cf. Bloodstein, 1995). It is also possible that speech sound disorders in children accompany neurogenic stuttering. Again there is no taxonomy.
After clarifying the neurological background and possible coexisting speech disorders, speech fluency can be examined by objective stuttering tests. A common objective measuring instrument to determine the stuttering severity is the SSI (Riley, 1994), the stuttering severity instrument which helps to examine the frequency of stuttering, the duration of stuttering moments and physical concomitants.
Additionally it can be helpful to analyze qualitative aspects of symptomatology, as well.
You can differentiate between clonic and tonic core symptoms: repetitions, which belong to the clonic stuttering symptoms, and prolongations and blocks which belong to the tonic stuttering symptoms. In most cases, neurogenic stuttering as well as idiopathic stuttering is characterized by both clonic and tonic stuttering symptoms. Only a minority of neurogenic stuttering individuals shows exclusively clonic stuttering symptoms or exclusively tonic stuttering symptoms. However in those cases, where clonic and tonic symptoms coexist, repetitions are often reported to occur more frequently than prolongations and blocks (cf. case studies of Lebrun & Leleux, 1985; Leder, 1996; McClean & McLean, 1985; Quinn & Andrews, 1977; Soroker et al., 1990; Stewart & Grantham, 1993; Tobin & Olsen, 1980; Van Borsel et al., 1998; Van Borsel, Van Der Made & Santens, 2003).
Clonic stuttering symptoms can occur in the form of sound repetitions, syllable repetitions, and whole word repetitions. However we need to keep in mind, that whole word repetitions especially those of polysyllabic words are more likely to be a form of avoidance behavior than a core symptom.
But is there anything that allows us to distinguish between neurogenic and developmental stuttering on the basis of symptomatology?
Some authors have suggested different characteristics of neurogenic stuttering. The following table summarizes characteristics Canter (1971) and Helm-Estabrooks (1993, 1998) have discussed on the bases of their clinical observations.
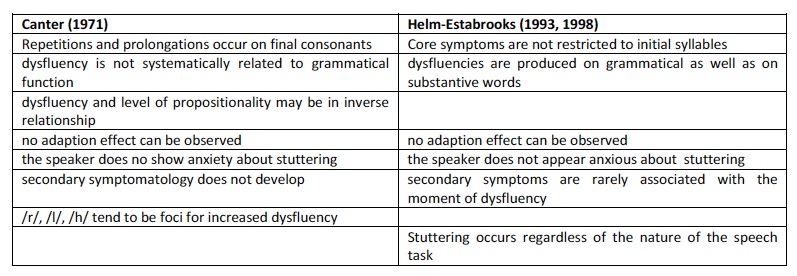
However the authors stress that presence of one or two of these characteristics cannot be considered as sufficient for diagnosing an individual with neurogenic stuttering. Rather, the identification of certain of these speech characteristics may help to raise the question of whether the fluency disorder might be neurogenic (cf. Canter, 1971).
As yet, no speech characteristics could be identified that allow a differential diagnosis to reliably differentiate between neurogenic or developmental stuttering. The strongest indicator is still a clear association with a neurological disorder or disturbance.
In addition to an objective stuttering measurement it is recommendable to administer a subjective test, such as the Overall Assessment of the Speaker's Experience of Stuttering (OASES - Yaruss & Quesal, 2006). It is based on the ICF model and "[...] was designed to supplement existing clincian-administered measures of the stuttering impairment" (ibid., 95). With its four sections it inquires: general perspectives about stuttering, affective behavioral and cognitive reactions to stuttering, functional communication difficulties, and the impact of stuttering on the speaker's quality of life.
On the basis of the qualitative and quantitative test results, treatment strategies can be chosen.
It is recommendable to start treating those aspects which affect the individual's life the most. If it is the accompanying speech disorder, the aphasia or the apraxia of speech, you can start treating that. If it is for example anxiety to speak, lack of self-confidence and/or impaired participation in every-day life due to the fluency disorder, you can start from there. If the speech fluency itself impacts the individual the most, you can start with direct stuttering therapy.
In the stage of therapy planning it is desirable to provide a target definition which considers both the patient's and the therapist's expectations, which might differ in some ways.
Working on speech fluency, different stuttering techniques can be used:
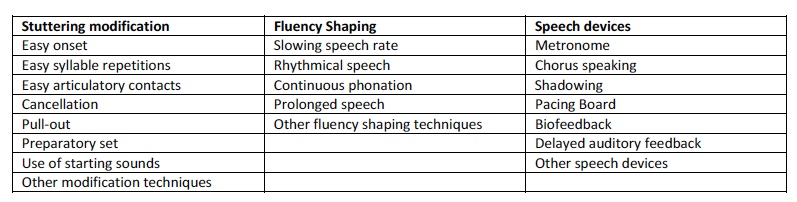
Research has shown that those methods used in developmental stuttering therapy can be suited for neurogenic stuttering therapy as well (cf. Koenig, 2009).
In order to assure transferring the use of those into every-day situations, enhance activities participation in communication situations, reduce psychological strain and negative impact of stuttering in every-day life, methods from stuttering therapy should be supplemented by psycho-social methods.
Working on both the speech factors and the psycho-social factors, meets the idea of the ICF best.
Thinking, once again, of Van Riper's metaphor of a complicated multidimensioned jigsaw puzzle of stuttering. It is apparent that there are still a lot of pieces that need to be added by further research to help us better understand this puzzling speech disorder called neurogenic stuttering. However previous and current research, practice and experience have contributed essentially to make the puzzle to what it is already -- an impressive entity, with very many parts that were already put together, which encourages us to treat and help neurogenic stuttering patients with our current knowledge as good as we can by now.
Contact: Dr. Kathrin Koenig Email: koenig1509@web.de
REFERENCES
BAUMGARTNER, J.; DUFFY, J. R. (1997): Psychogenic stuttering in adults with and without neurologic disease. Journal of Medical Speech-Lang Pathology, Vol. 5, 75-95.
BLOODSTEIN, O.: (1995) A Handbook on Stuttering. 5th Edition, San Diego, California: Singular Publishing Group, INC.
CANTER, G. J.: (1971) Observation on neurogenic stuttering: a contribution to differential diagnosis. British Journal of Disorders of Communication, Vol. 6, 139-143.
CURLEE, R. F.: (1995) Comments on "Neurogenic stuttering: An analysis and critique". Journal of Medical Speech-Language Pathology, Vol. 3, 123-124.
CHRISTMAN, S. S.; BOUTSEN, F. R.; BUCKINGHAM, H. W.: (2004) Perseveration and other repetitive verbal behaviors: functional dissociations. Seminars in Speech and Language -- Perservation in Neurogenic Communication Disorders. New York, Stuttgart: Thieme, Vol. 25, 295- 307.
DE NIL, F.; JOKEL, R.; ROCHON, E.: (2007) Etiology, symptomatology, and treatment of neurogenic stuttering. In: CONTURE, E. G.; CURLEE, R. F. (Hrsg.): (2007) Stuttering and related disorders of fluency. 3rd Edition, New York, Stuttgart: Thieme.
DE NIL, F.; ROCHON, E.; JOKEL, R. : (2008) Adult-onset neurogenic stuttering. In: MCNEIL, M.: (2008) Clinical management of sensorimotor speech disorders. 2nd Edition, New York: Thieme, 235-249.
FARMER, A.: (1975) Stuttering repetitions in aphasic and nonaphasic brain damaged Adults. Cortex, Vol. 11, 391-396.
FAWCETT, R. G.: (2005) Stroke-associated acquired stuttering. CNS Spectrums, Vol. 10(2), 94-95.
GRANT, A. C.; BIOUSSE, V.; COOK, A. A.; NEWMAN, N. J.: (1999) Stroke associated stuttering. Archives of Neurology, Vol. 56, 624-627.
GROHNFELDT, M.: (1992 b) Was ist "Erfolg" in der Stottertherapie?. Die Sprachheilarbeit, Vol. 37, 227-239.
HELM, N. A.; BUTLER, R; CANTER, G. J..: (1980) Neurogenic Acquired stuttering. Journal of Fluency Disorders, Vol.5, 269-279.
HELM-ESTABROOKS, N. A.: (1986) Diagnosis and management of neurogenic stuttering in adults. In: ST. LOUIS, K. O: (1986) The Atypical Stutterer -- Principles and Practices of Rehabilitation. Speech, Language and Hearing Series, Orlando: Academic Press, INC, 193-217.
HELM-ESTABROOKS, N. A.; HOTZ, G.: (1998) Sudden onset of "stuttering" in an adult: neurogenic or psychogenic? Seminars in speech and language, Vol. 19 (1), 23-29.
HELM-ESTABROOKS, N. A.: (1999) Stuttering associated with acquired neurological disorders. In: CURLEE, Richard F.: (1999) Stuttering and related disorders of fluency. New York: Thieme Medial Publishers, 2nd Edition, 255-268.
HORNER, J.; MASSEY, W.: (1983) Progressive dysfluency associated with right hemisphere disease. Brain and Language, Vol. 18, 71-85.
JOKEL, R.; DE NIL, L.; SHARPE, K. : (2007) Speech Dysfluencies in Adults with Neurogenic Stuttering Associated with Stroke and Traumatic Brain Injury. Journal of Medical Speech and Language Pathology, Vol. 15 (3), 243-261.
KOENIG, K.: (2006) Neurogenes Stottern -- Literaturanalyse und Erstellung informeller Materialien fuer die Erfassung individueller Auspraegungen des Stoerungsbildes. Unpublished diploma thesis, Technical University Dortmund.
KOENIG, K.: (2009) Moeglichkeiten und Grenzen in der Behandlung neurogenen Stotterns. Entwicklung, Evaluation und Anwendung eines Erhebungsinstrumentes. Dissertation. Technical University Dortmund.
LEBRUN, Y.; LELEUX, C.; ROUSSEAU, J.-J.; DEVREUX, F.: (1983) Acquired stuttering. Journal of Fluency Disorders, Vol. 8, 323-330.
LEBRUN, Y.; DEVREUX, F.; ROUSSEAU, J.-J.: (1986) Language and speech in a patient with a clinical diagnosis of progressive supranuclear palsy. Brain and Language, Vol. 27, 247-256.
LEBRUN, Y.: (1997) Adult-onset stuttering. In: LEBRUN, Y: (1997) From the brain to the mouth. Kluwer Academic Publishers, Dordrecht, Boston, London, 105-138.
LEDER, S. B.: (1996) Adult onset of stuttering as a presenting sign in a Parkinson Ian-like syndrome: a case report. Journal of communication disorders, Vol. 29, 471-478.
MANNING, W. H.: (2001) Clinical Decision Making in Fluency Disorders. 2nd Edition, Auckland: Singular.
MARKET, K. E.; MONTAGUE, J. C.; BUFFALO, M. D.; DRUMMOND, S. S.: (1990) Acquired stuttering. Descriptive data and treatment outcome. Journal of Fluency Disorders, Vol. 15, 21-33.
MARSHALL, R. C.; STARCH, S. A.: (1984) Behavioral treatment of acquired Stuttering. Autstralian Journal of human communication disorders, Vol. 12, 87-92.
McCLEAN, M.; McLEAN, A.: (1985) Case report of stuttering acquired in association with phenytoin use for post-head-injury seizure. Journal of Fluency Disorders, Vol. 10, 241-255.
NASS, R.; SCHRETER, B.; HEIER, L.: (1994) Acquired stuttering after a second stroke in a two-year-old. Developmental Medicine and Child Neurology. Vol. 36, 70-83.
QUINN, P. T.; ANDREWS, G.: (1977) Neurological stuttering -- a clinical entity? Journal of Neurology, Vol. 40, 699-701.
RENNER, J. A.: (1995) Erfolg in der Stottertherapie. Schriften zur Sprachheilpaedagogik, 6, Berlin: Edition Marhold.
RINGO, C.C.; DIETRICH, S.: (1995) Neurogenic Stuttering: An Analysis and Critique. Journal of Medical Speech Language Pathology, Vol. 3, 111-122.
ROSENBEK, J. C.: (1984) Stuttering secondary to Nervous System Damage. In: CURLEE, R. F.; PERKINS, W. H. (1985): Nature and Treatment of Stuttering: New Directions. San Diego, College-Hill, 31-48.
ROSENFIELD, D. B.; VISWANATH, N. S.; CALLIS-LANDRUM, L.; DI DANATO, R.; NUDELMAN, H. B.: (1991) Patients with Acquired Dysfluencies: What they tell us about developmental stuttering. In: PETERS, H. F. M; HULSTIJN, W.; STARWEATHER, C. W.: (1991) Speech Motor Control and Stuttering. International Congress Series 950. Amsterdam: Excerpta Medica.
SOROKER, N.; BAR-ISRAEL, Y.; SCHECHTER, I.; SOLZI, P.: (1990) Stuttering as a Manifestation of Right-Hemispheric Subcortical Stroke. European Neurology, Vol. 30, 268-270
STEWART, T.; GRANTHAM, C.: (1993) A case of acquired stammering: the pattern of recovery. European Journal of Disorders of Communication, Vol. 28, 395-403.
STEWART, T.; ROWLEY, D.: (1996) Acquired stammering in Great Britain. European Journal of Disorders of Communication, Vol. 31, 1-9
TIPPETT, D. C.; SIEBENS, A. A.: (1991) Distinguishing psychogenic from neurogenic dysfluency when neurologic and psychologic factors coexist. Journal of fluency disorders, Vol. 16, 3-12.
TOBIN, H. W.; OLSEN, B. D.: (1980) Adult Onset Stuttering -- A Case Report. The Journal of the Maine Medical Association, Vol. 71, 8-11.
VAN BORSEL, J.; VAN DER MADE, S.; SANTENS, P.: (2003) Thalamic stuttering: A distinct clinical entity? Brain and Language, Vol. 85, 185-189.
VAN BORSEL, J.; VAN LIERDE, K.; OOSTRA, K.; EECKHAUT, C.: (1997) The differential diagnosis of late-onset stuttering. In: Lebrun, Y.: (1997) From the brain to the mouth -- Acquired Dysarthria and Dysfluency in Adults.
VAN RIPER, C.: (1982) The nature of stuttering. Englewood Cliffs N.J.: Prentice Hall.
YAIRI, E.; GINTAUTAS, J.; AVENT, J. R.: (1981) Dysfluent speech associated with brain damage. Brain and Language, Vol. 14, 49-56.
YARUSS, J.S.; QUESAL, R. W.: (2004) Stuttering and the international Classification of Functioning, Disability, and Health (ICF): An update. Journal of Communication Disorders, Vol. 37, 35-52.
YARUSS, J.S.; QUESAL, R. W.: (2006) Overall Assessment of the Speaker's Experience of Stuttering (OASES): Documenting multiple outcomes in stuttering treament. Journal of Fluency Disorders, Vol. 31, 90-115.
ZUECKNER, H.; EBEL, H.: (2001) Erworbenes psychogenes Stottern bei Erwachsenen: Diagnostische und differenzialdiagnostische Aspekte. Sprache, Stimme, Gehoer, Vol. 25, 110-117.