Differential Diagnosis of Stuttering and Self-Referral
 |
About the presenter: Dr Marie-Claude Monfrais-Pfauwadel is an MD and ENT (graduated from CHU Broussais in Paris), Phoniatrician, DEA in formal linguistics and phonetics (Paris 7), and DEA in clinical psychology ( Paris 6). She participated to the first SFA International Workshop in 1985 and has been a Member of the Fluency Committee of IALP since 1986. Among the founding members of IFA, she organized and hosted the first World Congress of IFA in 1991 in Paris (Saulx- les Charteux). Past President of the French Phoniatric Medical Society. Assistant to Dr Chevrie-Muller for several years at Laboratoire de recherche sur le Langage (INSERM) at Hospital la Salpetri�re (Neurology). Created the Laboratory of Voice Speech and Swallowing Disorders of Assistance-Publique in Paris in 1986 ; now situated in European Hospital Georges Pompidou. Created the first medical Stuttering Clinic at Hospital Europ�en Georges Pompidou in January 2000. Currently teaches Neurophysiology of Speech to future linguists and phoneticians (University Denis Diderot) and Fluency disorders and Stuttering assessment and management to future phoniatricians (Leonard de Vinci Medical School � University Paris 13). Author of several books on voice (1986), stuttering (1986) and a textbook for speech pathology students about stuttering (2000). Co-author of many books and textbooks about voice, speech motor control and communication modeling. |
Differential Diagnosis of Stuttering and Self-referral
by Marie-Claude Monfrais-Pfauwadel
from France
An experience that lasted three years and included 300 new patients in a recently opened Medical Stuttering Clinic at Hospital Georges Pompidou in Paris led to some surprising and interesting clinical findings. The original purpose of this clinic was to emphasize diagnosis, counseling, planning of treatment strategies for stuttering inside a general hospital and to provide a service that did not yet exist. The idea of clinical research soon followed as the database grew quickly (100 new patients each year for a once a week consultation). One of our aims was to establish complete and standardized questionnaires and assessment forms in French and then to validate those instruments to measure clinically the efficacy of treatment.
Stuttering treatment is not typically provided in the hospital clinic and all patients are referred to specialized therapists if available, or at least they are counseled. The surprise, as we began to analyze our data base, was to realize that many patients who referred themselves, thinking that they were "real stutterers", were actually "atypical" stutterers. In fact, many of those patients had one or more neurological symptoms or disorders that were interfering with their speech, which in fact, was very disfluent. Thus the challenge became to extend the clinical routine to include neurological clinical investigations of speech motor control -- first of all through the questionnaires, assessments and case history, then in strengthening our relationships with neurological teams, mainly specializing in movement disorders.
The medical stuttering clinic:
- The unique setting and surroundings provided an opportunity to explore a new concept in France.
- A multidisciplinary team consisting of one person, the author (who is an MD, ENT-phoniatrician, but also a phonetician and psychologist)
- The patients: the clinic was opened primarily on the basis of self-referral and on the model of symptom-based clinics ( such as migraine clinics, tinnitus clinics, etc...); out of 300 patients, 244 self-referred "off the street."
The first overall statistics:
- Ratios of male/female 4:1
- Adults/children (142 adults, 158 children)
- Family history (42% with at least one sibling)
- Handedness (15, 6% left handed)
- Age of onset, relapse and recoveries, language impairments, Attention Deficit Disorders, sleep disorders (somnambulism, catalepsy) are still to be computed, as well as the complex relationships between disorders.
- Neurological disorders are the topic of this presentation.
Methodology
The speech and language protocols used for recording and analyzing stuttered speech were the same already standardized protocols used in our laboratory for dysarthrias
- counting
- phonetically balanced passage and lists, to be read and/or repeated
- spontaneous speech
- sustained vowels
- S/Z ratio
- syllables (consonant paradigm)
- repeated rapid speech - diadokokinesis
- story-telling (language level) etc.
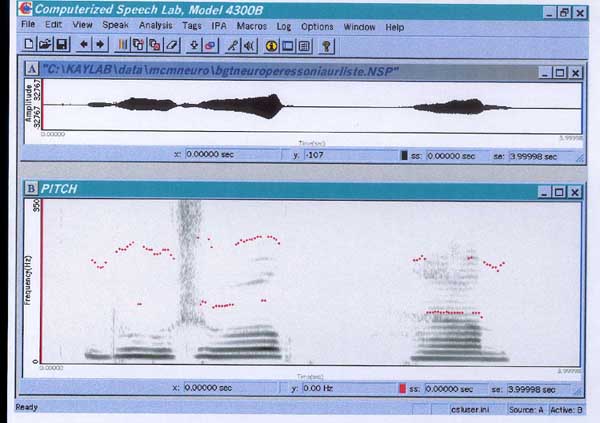
This information was recorded in a soundproof room on a DAT tape-recorder. The acoustic and phonetic analysis of voice and speech were performed with Kay-Elemetrics CSL hardware.
For the stuttering assessment, all patients underwent the same clinical procedure: answer a lengthy questionnaire (one for children, another one for adults) about onset, case history, family history, handedness, history of neurological disorders, attitudes, previous attempts of rehabilitation and treatment (and outcome), drug treatments, more precise questionnaires in case of attention deficit disorders, language impairment, neurological complaints, lateralization problems, etc In case of neurological findings, if not yet explored, a complete neurological clinical examination including appropriate neuro-imagery was prescribed.
About the different neurological diagnosis encountered:
173 patients had one to several different neurological disorders, many of which could be related to the "speech impairment." Those different disorders are listed below, illustrated, if available by sound samples and matching spectrograms. For each patient you will hear and look at a sustained "A" and at least one word of the standardized list of words used for the exploration of dysarthrias (Dr Chevrie-Muller), usually "bonjour" (good-morning in French), unless otherwise specified.
This paper presents a few of those cases where patients either had been diagnosed as "typical" stutterers, at times within a context of other problems, or patients who genuinely believed they were "just stutterers" although there was clear evidence of neurogenic disfluent speech.
1 Tourette, maladie des tics
In our series, we diagnosed 4 real cases of Tourette (first diagnosis) (1.2% of our cases -- usual incidence 0.02%) and 21 cases (7%) of maladie des tics.
Tics are brief, repetitive, purposeless, non-rhythmic, involuntary movements or sounds that tend to occur in bursts or "bouts." Simple tics involve one muscle group or one simple sound. Simple vocal tics include throat-clearing sounds, grunting, sniffing, and coughing. They can be suppressed for short periods of time. Tics are primarily related to the prominent areas of the somatic motor representation. Complex tics involve a coordinated movement produced by a number of muscle groups (complex motor tic) or a linguistically meaningful utterance or phrase (complex vocal tic).
The Maladie de Gilles de la Tourette is of a more complex nature and involves multiple motor and one or more vocal tics. Onset occurs before age 18, typically between the ages of 2 and 15 (mean age 6.5). The prevalence is 1 case per 1000 population; genetic factors are of 75% with bilineal transmission in 25% of the cases. Tics occur many times a day, nearly every day. They vary in location, frequency and complexity over time. Vocal tics begin 1 to 2 years after motor tics. 50% of people with Tourette's also have Attention Deficit Hyperactivity Disorder (ADHD). Stuttering or atypical stuttering is very frequent. Diagnosis does not require a radiological or laboratory workup and was fairly easy and evident for the patients who came at the clinic. It is sometimes not well accepted by parents until they discover that treatment provides real relief. Treatment may include clonidine, benzodiazepines, haldol, risperdal, clozapine, reserpine, along with speech, behavioral rehabilitation and counseling.
2 Strokes-- Phonemic aphasia
3 cases of adult-onset stuttering after a stroke (cerebral vascular accident) within a context of aphasia (phonemic aphasias)
2 cases of congenital hemiplegia with related aphasia
The following patient is a 75 year old man, right handed, who stuttered as a child. After a cerebro-vascular hemorrhage (in the region of the sylvian artery), he became aphasic and again began stuttering. He is a music composer and as you can hear and see, his prosody is really well maintained. The "disfluencies" are easy and the voice is melodious.
Sound file:
Sound file:
3 Epilepsy
16 cases were under treatment for seizures and 8 additional cases had a history seizures accompanying a high fever during infancy. Some still had seizures, even with treatment. There were no Landau -Kleffner syndrome patients among our patients, up to this point.
The following woman, age 40, left-handed, started stuttering at the age of 8 at the same time her first seizures occurred. She is successfully treated for her epilepsy, but remains a severe stutterer. The stuttering problem shows little variation with the emotional content of the speech situation. Stuttering increases during the aura period associated with her seizures.
Sound file:
Sound file:
4 Abnormal movements:
Dystonia are sustained muscle contractions that can be focal, segmental, hemi or generalized. They cause twisting movements (opposing muscles) and can occur at rest (unlike stuttering). There exists a paroxysmal (convulsive) form. The localization of the dystonia itself can interfere with the motor execution of speech (Molt, Jankovic and Fahn). These patients represent 12% of our cases! Symptoms are primarily tongue dystonias, but also mouth, lips or jaw dystonias.
Tongue dystonia: 10 cases -- this type of dystonia could interfere greatly with the production of speech.
The following patient, age 40, pharmacist, with multiple dystonias so far undiagnosed; his speech was becoming increasingly slurred.
Sound file:
Sound file:
Sound file:
Focal Dystonias
Facial dystonias: 16 cases, plus 3 cases of head dystonias
The following is a young woman of 22, right handed, uttered this speech sample . Her stuttering severity score rated 6/7 on the Cooper scale; she also has a moderate ADD and had been diagnosed with a language impairment during childhood.
Sound file:
Sound file:
Spasmodic torticollis
4 cases
Dystonia-dyskinesias
2 cases
Volitional dyskinesias:
4 cases
5 Cerebellar pathology
The cerebellum does not initiate muscular activity but coordinates it so that movements are fluid. It coordinates agonist and antagonist muscles and maintains muscle tone and equilibrium. It receives information from muscles, joints, the cortex and inner ear and contains numerous feedback loops.
Ataxia: 3 cases, among which was one of the following sisters
Four sisters, aged 14 to 23, all of them diagnosed as developmental stutterers. The father had been a stutterer during his childhood. In addition, four cousins (father's sister's children) are stutterers. The youngest girl was diagnosed with cerebellar atrophy at age 10 (with IRM evidence). They all have +/- degrees of focal dystonia. None can ride a bicycle.
The father, an opera chorus singer, had been a stutterer as a child. The mother is remarried and has another child from her new husband, totally symptom free
Sound file:
Sound file:
Stephanie, the eldest, age 23 is tbe mother of a 2 year old boy, non stutterer so far Stephanie's sustained A vowel spectrographic analysis
Sound file:
no sound file
Audrey, the second youngest has marked symptoms. She has been a stutterer as long as she can remember Audrey's sustained A vowel spectrographic display
Sound file:
Sound file:
Elodie, 18 years old, was the first one to consult for "stuttering." Referred by her father-in-law, (one of my laryngectomy patients). Elodie's sustained A vowel spectrographic display
- Shortness of breath
- Instability next to tremor
- Instability of the harmonics and lack of timbre
Sound file:
Sound file:
Aurelie's sustained A vowel spectrographic display. She had been diagnosed in a children's hospital as "cerebellar" as there was a cerebellar atrophy on the imaging at the age of 13. Also diagnosed with language impairment, dysgraphia. High reactionnal attitude score
Sound file:
Sound file:
Those four sisters consider themselves to be stutterers and the two youngest sisters are now receiving speech therapy. None of them can ride a bicycle. Genetic diagnosis is under way. Their dystonia seems to be dopamine sensitive.
6 Closed head injury
15 cases including 3 who had been in a coma -- in 3 other cases a childhood stuttering has been reactivated following the trauma
7 Meningitis:
5 cases, all prior to the onset of stuttering.
8 Agenesis of corpus callosum:
1 case
8 Wilson's disease
An excess of copper in the blood (inherited disorder of copper metabolism; autosomal recessive transmission; prevalence 1/30000) causes hepatolenticular degenerescence . Dysarthria (the corpus striatum is dysfunctioning), involuntary movements, bilateral tremor of the extremities, spasticity, drooling, dysphagia, velar paresis, and seizures are among the typical symptoms.
case - undiagnosed while in speech therapy for years, a woman age 32. The typical velar consonants modifications (repetition) that you will hear were totally consistent and could happen within words as well as in the initial position during speech, and in reading, as well as in spontaneous speech. The word "spectacle" and the word "carre" in the attached speech samples demonstrate blockages that can last for more than 15 seconds.
Sound file:
Sound file:
Sound file:
9 Nuclear ictus
22 cases
10 Cerebral palsy
12 cases including a case of athetosis, 2 cases of craniostenosis and one case of hydrocephalia
A young adult of 18 with mild athetosis.
no sound file
Sound file:
The follow-up
As much as possible (and manageable) patients were asked to return in six months or a year for retesting and then at least once a year. Many patients returned on the second or third meeting with their speech therapist for further advice and counseling on the techniques and strategies for rehabilitation.
Patients with drugs prescription were asked to report more often, by phone or e-mail if living far from the hospital (and not reporting to a neurological team).
These examples led us to some theoretical thoughts about motor impairment:
In apraxia of speech, the primary contributor is impairment at one or more level of motor processing.
In dysarthrias, impairments occur at both the motor level and the sensory-motor feedback level.
In stuttering, the reference is to a mainly motor level of impairment; however there seems to be impairment in the timing of individual articulators or the temporal sequencing among serial multiarticulate movements that occur prior to the level of sensorimotor execution (Caruso and Strand).
Some theoretical thoughts about coordination of movements
A coordinated movement requires :
- Appropriate muscle selection
- Appropriate muscle tension
- Precise timing and sequencing or articulatory dynamics
These may be lacking in stuttering speech as well as in dysarthrias, as different types of motor speech disorders may be associated with different types of coordination problems :
- In apraxia of speech, patients have difficulty programming the events necessary for coordinated movement
- In cerebral palsy, patients (mainly in athetosis and chorea-athetosis) are unable to regulate the magnitude or the degree of muscular tension
- In stuttering, patients may have a restricted ability to precisely time or sequence individual structures to work in synchronicity with each other
Differential diagnosis of stuttering or atypical stuttering (According to Ludlow and Monfrais-Pfauwadel)
Some parting questions
- Is there a clear border line between dysarthric disfluencies and stuttering ?
- Is there such a diagnosis as "typical stuttering?"
- Where is the line between dysarthrias and stuttering, as appropriate muscle selection, appropriate muscle tension and precise timing or sequencing of articulator dynamics may lack in both instances?
- What is the sensory part of the global impairment of movement in stuttering?
- Should every stutterer undergo a medical/and or a neurological or phoniatric examination, to rule out if any neurological disorder is underlying the clinical findings?
- Should every stutterer undergo a precise instrumental analysis of disfluencies?
- Are those patients to be treated differently?
- Could "typical stutterers" benefit by some of the neuropharmacology used for the pure neurological patients?
- How can we effectively collaborate with neurologists? Why don't neurologists acknowledge that there are neurological stutterings, though they ask for speech rehabilitation for the very patients they send us for "atypical stuttering"?
ADDENDUM
Nosological classification of disfluencies (Monfrais-Pfauwadel 1990 and 1995)
- stuttering
- spasmodic dysphonia
- extrapyramidal dysarthrias
- Parkinson's disease
- Steele-Richardson-Olewski syndrome,
- choreas and athetosis.
- cerebellar syndromes and ataxias dystonias specially focal
- volitional dyskinesias of intention
- myoclonias of the larynx,
- tics and Gilles de le Tourette syndrome
- apraxias of speech (Kent, Lebrun) .
- anarthrias
- Phonemic disintegration syndrome
- word retrieval disorders in aphasias
- substitutive phonations in a laryngeal speech
- esophageal speech
- tracheo esophageal speech
- external vibratory devices for alaryngeal patientsdysarthrias
- extrapyramidal dysarthrias
Bibliography
- Ackermann, H., Hertrich, I., Ziegler, W., Bitzer, M., & Bien, S. (1996). Acquired dysfluencies following infarction of left mesiofrontal cortex. Aphasiology, 10, 409-417.
- Adams, M.R. and Runyan, C.M. : Stuttering and fluency : exclusive events or points on a continuum ?, Journal of Fluency Disorders, 1981, 6, 197-218.
- Adams, M.R., Freeman, F.J. and Conture, E.G :Laryngeal dynamics of stutterers in Curlee, R.F. and Perkins W.H. (edits) Nature and treatment of stuttering. New directions, Taylor and Francis, 1985, 89-129.
- Alfonso, P. Implications of the concepts underlying task dynamic modeling on kinematic studies of stuttering, Haskins Laboratories Status Report on Speech Research, 1991, 107, 93-110.
- Alfonso, P., Kalinowski and Story, R. The effect of speech motor training on stutterers� speech physiology, Haskins Laboratories Status Report on Speech Research, 1991
- Andy, O. J., & Bhatnagar, S. C. (1992). Stuttering acquired from subcortical pathologies and its alleviation from thalamic perturbation. Brain and Language, 42, 385-401.
- Andy, O.J., and Bhatnagar, S.C. (1991). Thalamic-induced stuttering (surgical observations). Journal of Speech and Hearing Research, 34, 796-800.
- Ardila, A., & Lopez, M. V. (1986). Severe stuttering associated with right hemisphere lesion. Brain and Language, 27, 239-246.
- Aronson, A. : Clinical voice disorders, Arnette �dit., Paris,1980
- Baratz, R., & Mesulam, M. M. (1981). Adult-onset stuttering treated with anticonvulsants. Archives of Neurology, 38, 132.
- Bijleveld, H., Lebrun, Y., & Van Donden, H. (1994). A case of acquired stuttering. Folia Phoniatrica, 46, 250-253.
- Byrne, A., Byrne, M. K., &
- Brady, J. (1991). The pharmacology of stuttering: A critical review. American Journal of Psychiatry, 148, 1309-1316.
- Chevrie-Muller, C. : �tude du comportement laryng� chez les b�gue par la m�thode glottographique. [Stutterer's laryngeal behavior: A glottographic study]. Revue Laryngologie 10 (1991) 763-764
- Dalton, P. & Hardcastle, W. (1989). Disorders of fluency and their effects on communication. London: Elsevier North Holland.
- Dietrich, S., Barry, S.J., & Parker, D. (1995). Middle latency auditory responses in males who stutter. Journal of Speech and Hearing Research, 38(1), 5-18.
- Farmer, A. (1975). Stuttering repetitions in aphasic and nonaphasic brain damaged adults. Cortex, 11, 391-396.
- Grant, A. C., Biousse, V., Cook, A. A., & Newman, N. J. (1999). Stroke-associated stuttering. Archives of Neurology, 56, 624-627.
- Gregory, H.H Stuttering, differential evaluation and therapy, Pro-Ed, Austin, Texas, 1986.
- Helm, N. A., & Butler, R. B. (1980). Neurogenic acquired stuttering. Journal of Fluency Disorders, 5, 269-279.
- Helm, N. A., Butler, R. B., & Benson, D. F. (1978). Acquired stuttering., Neurology, 28,1159-1165.
- Helm-Estabrooks, N. (1986). Diagnosis and management of neurogenic stuttering in adults. In K. O. StLouis (Ed.), The atypical stutterer (pp. 193-217). Orlando: Academic Press. 2
- Helm-Estabrooks, N., Yeo, R., Geschwind, N., Freedman, M., & Weinstein, C.(1986). Stuttering: Disappearance and reappearance with acquired brain lesions. Neurology, 36, 1109-1112.
- Howell, P., Sackin, S., & Rustin, L. (1995). Comparison of speech motor development in stuttering and fluent speakers between 7 and 12 years old. Journal of Fluency Disorders, 3, 243-255.
- Ingham : Functional-lesion investigation of developmental stuttering with positron emission tomography (vol 39, pg 1208, 1996) Journal of Speech Language and Hearing Research 40: 1(FEB 1997),182
- Kelly, EM., Smith, A., & Goffmann, L. (1995). Orofacial muscle activity of children who stutter: A preliminary study. JOURNAL OF SPEECH AND HEARING RESEARCH, 38, 1025-1036
- Kent, R.D., Rosenbeck J.C., : Prosodic disturbance and neurologic lesion, Brain and Language, 1982, 15, 259-291.
- Kent, R.D.: Stuttering as a temporal programming disorder in R. Curlee and W. Perkins, eds, : Nature and treatment of stuttering, new directions, 283-301, San-Diego, College Hill Press, 1984.
- Koller, W. C. (1983). Dysfluency (stuttering) in extrapyramidal disease. Archives of Neurology, 40, 175-177.
- Lebrun, Y. (1996). Cluttering after brain damage Journal of Fluency Disorders, 21 (3/4), 289-295.
- Lebrun, Y., Leleux, C., & R�tif, J. (1987). Neurogenic stuttering. Acta Neurochirurgica, 85, 103-109.
- Lebrun, Y., Leleux, C., Rousseau, J-J, & Devreux, F. (1983). Acquired stuttering. Journal of Fluency Disorders, 8, 323-330.
- Leder, S. B. (1996). Adult onset of stuttering as a presenting sign in Parkinsonian-like syndrome: A case report. Journal of Communication Disorders, 29, 471-478.
- Leder, S.B. (1996). Adult onset of stuttering as a presenting sign in a parkinsonian-like syndrome: A case study. Journal of Communication Disorders, 29(6): p471-478.
- Levelt, W.J.M. : Speaking From intention to articulation. Cambridge, MA: MIT Press, 1989
- Lewis, E.K. The structure of disfluencies behaviors in the speech of adults stutterers. Journal of Speech and Hearing Research, 34, 1991.
- Ludlow, C. and Cooper, J.(eds) : Genetic aspects of speech and language disorders Academic Press edit., New York ,1983.
- Ludlow, C.L. and Braun A.� Research evaluating the use of neuropharmalogical agents for treating stuttering: possibilities and problems, Journal of Fluency Disorders, 1993, 18, 169-182.
- Ludlow, C.L., & Braun, A. (1993). Research evaluating the use of neuropharmacological agents for treating stuttering: Possibilities and problems Journal of Fluency Disorders, 18, 169-182.
- Ludlow, C.L., and Dooman, A. : Genetic aspects of idiopatic speech and language disorders, Otolaryngologic clinics of North America, 25, 5, 979-994, 1992.
- Monfrais-Pfauwadel M.-C.: Pour une classification nosologique des disfluences de la parole, M�moire de DEA de Phon�tique, Universit� Paris VII, 1990.
- Monfrais-Pfauwadel M-C. : Les disfluences autres que celles du b�gaiement, Revue de Laryngologie, Bordeaux, 1995.
- Monfrais-Pfauwadel M-C. Le concept de fluence verbale, Les cahiers de Fontenay, 1994, 75, 89-98
- Monfrais-Pfauwadel, M.C.: R�cidives et risques de r�cidive chez l�adulte b�gue, Questions de Logop�die, Bruxelles,1998.
- Monfrais-Pfauwadel, M.C : Un manuel du b�gaiement, Solal edit., Marrseille, 2000
- Perkins, W.H., Kent, R.D. et Curlee, R.F. : A theory of neuropsycholinguistic function in stuttering. Journal of Speech and Hearing Research, 1991, 34, 734-752.
- Peters H. et Hulstijn W. : Speech Motor Dynamics in Stuttering, Springer Verlag edit, Amsterdam,1987.
- Peters, H. : Stuttering: Studies in speech motor behavior, Druk: Krips Repro Meppel, Thesis Nijmegen, 1987.
- Peters, H. et Boves, L. (1988) Coordination of aerodynamic and phonatory processes in fluent speech utterences of stutterers, Journal of Speech and Hearing Research, 31, 352-361.
- Peters, T., & Guitar, B. Stuttering: An integrated approach to its nature and treatment. Baltimore: Williams & Wilkins. 1991, 1986
- Pfauwadel, M.C : Le b�gaiement de l'enfant. [Stuttering in children]. Medicine et Enfance 8:1 (1988) 47-49
- Pfauwadel, M.C. : Etre B�gue, Le Hameau �dit., Paris, 1986.
- Preus, A. (1981). Identifying Subgroups of Stuttering. Oslo, Norway: Universitetsforlaget.
- Rieber, R.W., Breskin, S., & Jaffe, J. (1972). Pause time and phonation time in stuttering and cluttering. Journal of Psycholinguistic Research 1, 149-154.
- Ringo, C. C., & Dietrich, S. (1995). Neurogenic stuttering: An analysis and critique. Journal of Medical Speech-Language Pathology, 3, 111-122.
- Rosenbeck, J.� Apraxia of speech, the relationship to stuttering, Journal of Fluency Disorders , 1980, 5, 255-267.
- Rosenbek, J., Messert, B., Collins, M., & Wertz, R. T. (1978). Stuttering following brain damage. Brain and Language, 6, 82-96.
- Rosenfield D.B. : Stuttering, Current problems in Pediatrics, 1982, 12, 1-27.
- Rosenfield D.B. and Goodglass H. : Dichotic testing of cerebral dominance in stutterers, Brain and language, 1980, 11, 170-180.
- Scherer, K.�and Darby Speech evaluation in psychiatry, Grune & Stratton edit, New York, 1981
- Shapiro, D.A. : Stuttering intervention, Pro Ed edit, Austin Texas, 1999.
- Smith, A. Neural drive in stuttering, , Journal of Speech and Hearing Research 1989,32,252-264.
- Smith, A., Denny, M., Shaffer, L. A., Kelly, E. M., & Hirano, M. (1996).: Activity of intrinsic laryngeal muscles in fluent and disfluent speech. , Journal of Speech and Hearing Research JH, 39, 329- 348.
- St. Louis, KO (ed) (1986) The Atypical Stutterer: Principles And Practices of Rehabilitation. Orlando, FL: Academic Press.
- Stansfield J, (1990) Prevalence of stuttering and cluttering in adults with mental handicaps.J Ment Defic Res, 34 ( Pt 4) 287-307
- Starkweather W.: Fluency and Stuttering, Prentice Hall edit, New-Jersey, 1987.
- Stemberger,J. Glottal transparency, Phonology, 10, 1993, 107-138.
- Sussman, H.M., Mac Neilage, P.F. : Hemispheric specialization for speech production and perception in stutterers, Neuropsychologica, 1975, 13, 19-27.
- Teitler, N�. Phonologie de la syllabe dans le b�gaiement M�moire de DEA de Phon�tique, Universit� de Paris VII, 1998.
- Thacker, R.C., and DeNil, L.F. (1996). Neurogenic cluttering. Journal of Fluency Disorders 21, 227-238.
- Van Borsel, J., Van Lierde, K., Van Cauwenberge, P., Guldemont, I., Van Orshoven, M. (1998). Severe acquired stuttering following injury of the left supplementary motor region: a case report. JOURNAL OF FLUENCY DISORDERS, 23, 49-58.
- Van Hoot A., Estienne, F. Les b�gaiements, Masson �dit., Paris, 1996.
- Van Lieshout, PHHM. , Hulstijn, W.� and Peters, HFM.� From planning to articulation in speech production What differentiates a person who stutters from a person who does not stutter�? Journal of Speech and Hearing Research, 1996, 39, 3, 546-564.
- Van Riper, C. (1970). Stuttering and cluttering. Folia Phoniatrica 22, 347-353.
- Van Riper, C. : The nature of stuttering (2nd edit.), Prentice Hall edit., Englewood Cliffs, N.J., 1982. 7
- Whitaker, H.A. Phonological processes and brain mechanisms, Springer Verlag, New York, 1988.
- Wingate M.E. : Stuttering, theory and treatment, Irvington Publishers edit., New York, 1976.
- Wingate M.E. : The structure of stuttering, a psycholinguistic study. Springer Verlag, New York, 1988.
- Wingate, M.E. : Criteria for stuttering, Journal of Speech and Hearing Research, 1977, 20, 596-607.
- Wingate, M.E. : The immediate source of stuttering : an integration of evidence, Journal of Communication Disorders, 1977, 10, 45-53.
- Zellner, B. : Caract�ristiques du d�bit de parole en fran�ais, Th�se de Doctorat, Universit� de Lausanne, 1998.
- Zellner-Bechel, B. : H�sitation et b�gayage �tude des occurrences de disfluences verbales. M�moire de D.E.A., Universit� de Paris 7, 1991.
- Zimmermann, G. : Articulatory dynamics of fluent utterances of stutterers and nonstutterers. Journal of Speech and Hearing Disorders, 1980, 23,108-121.
- Zimmermann, G. : Stuttering, a disorder of movement, Journal of Speech and Hearing Research, 1980c, 23, 122-136.
September 2, 2002