Auditory Sidetone Paradigms for Treating Stuttering: From Wollensak To Speecheasy
 |
About the presenter: Richard M. Merson received his Ph.D. from the University of Wisconsin, Madison, in 1970. He subsequently completed a clinical and research fellowship at the Mayo Clinic (70-72) in Rochester, Minnesota. Thereafter he was the Head of the Speech-Language Pathology Clinic at Washington Unversity in St. Louis, Missouri, and then Director of the Speech Pathology and Audiology Clinics at Hahnemann University Hospital in Philadelphia, Pennsylvania, before coming to William Beaumont Hospital (1989) in Michigan. He is currently Coordinator of Clinical Research and Special Clinical Projects in the Speech-Language Pathology Department of William Beaumont Hospital in Royal Oak, Michigan. Dr. Merson is also a bioscientific member of the Medical Staff at William Beaumont Hospital. He divides his professional time between clinical practice and clinical empirical research on diagnostic and treatment strategies for communication disorders.He has published and lectured in the areas of neurogenic communication disorders, including Stuttering , Spasmodic Dysphonia, Vocal Paralysis, and Dysarthria (i.e. Parkinson's, Multiple Sclerosis) . |
Auditory Sidetone and the Management of Stuttering: From Wollensak to SpeechEasy
by Richard M. Merson
from Michigan, USA
"Speak the speech I pray thee as I pronounced it to you, trippingly on the tongue: but if you mouth it as many of your players do, I had as lief the town-crier spoke my lines. Nor do not saw the air too much with your hand , thus, but use all gently; for in the very torrent, tempest and as I may say the whirlwind of passion, you must acquire and beget a temperance that may give it smoothness ..."
Hamlet, Scene II William Shakespeare circa 16th Century
Introduction
Shakespeare glorified the power and passion of oratory and like many 21st century speech-language pathologists succumbed to "praying" that his subjects speak more smoothly, without sawing the air too much or becoming overwhelmed by the whirlwind of passion in verbal performance. As a clinical speech-language pathologist I have found my self reiterating Shakespeare's advice to many patients who must learn to manage their stuttering. When traditional therapy, counsel, instruction and praying gives way, a good electronic auditory sidetone device is not a bad idea. I much prefer the give and take of hardcore individual therapy that seeds the growth of fluency and finally gives way to confident verbal communication. However, when your caseload of secondary stuttering includes all ages and severities you must have a large repertoire of treatment strategies.
Historic Perspective
I like telling my patients that Socrates was the first to recommend auditory sidetone for persons who stutter. Socrates , as I tell the story, would urge the PWS (person who stutters) to go to the seashore and place a large conch shell to their ear and speak as they listened to the roar of the surf. Ann Dewar (1979) would later call this her Edinburg Masker. The Edinburg Masker presents a voice-actuated white noise that distracts the speaker or perhaps makes it difficult to focus on their own stuttering. Earlier in the 1950's and 60's as electronics became an integral part of our popular culture and the concepts of cybernetic feedback as an exciting sensorimotor research topic blossomed, auditory sidetone as a treatment for stuttering became a natural outgrowth .
A large number of clinical and experimental investigations were carried out in Europe and America during the 1950's through the 1990's using auditory sidetone stimuli to determine their fluency evoking effects on PWS as well as their fluency disruptive effects on persons who did not stutter. In Dr. Charles Van Riper's 1971 text , "The Nature of Stuttering" he dedicated an entire Chapter including over a 100 references on " Stuttering as the Result of Disturbed Feeback". There have been a number of auditory stimuli used on PWS to evoke fluency and they have included masking noises, metronome paced tones, distorted speech , delayed speech , choral speech, or combinations of these stimuli. The most effective auditory sidetone reported in the research and through much clinical concensus is delayed speech feedback
Briefly, when speech is fed back to a speaker via earphones at 75 to 100 milliseconds delay (one tenth of a second), the speaker will automatically (passively) slow their rate of utterance, flatten their intonation , prolong their words and/or raise their speech volume to cope with the competing signal. This effect is referred to as the DAF (delayed auditory feedback) effect. It is not a uniform effect among all PWS or all persons who are fluent. I have used DAF on many professional broadcasters who have no speech effect. They are used to listening to auditory sidetone ( i..e producers shouting instructions through earphones while they are broadcasting) and ignoring its potential effect on their own speech. In the same way PWS may become accustomed to the DAF and learn to ignore the signal and loose the fluency evoking effects. We also know from a number of clinical studies using DAF that binaural auditory sidetone is more effective than monaural . Further, some individuals are more susceptible or responsive to auditory sidetone speech effects. Finally, the speech effects of auditory sidetone are not easily generalized, when the sidetone is removed.
The early use of auditory sidetone in the 1950's was performed in the research laboratory with magnetic audiotape recorders. During the 1960's the better audiotape recorders ( i.e. Wollensak) could be used with magnetic tape loops or the public address outlet of the recorder to effect a random delayed auditory signal. The Wollensak tape recorder was the first auditory sidetone device that I used and while the signal could not be altered it had its standard effect with large binaural circumoral earphones. Eventually electronic circuits could be built to effect auditory sidetone for which the delays could be adjusted.
Most of the units required binaural earphones and a good size microphone with a rather klutsy box of electronics. The auditory sidetone units today have minature microphones, or lapel mics with smaller light weight earphones or earpieces and can be played through speakers as well. The Kay Elemetrics Corporation has an excellent portable auditory sidetone unit (The Facilitator) that Dr.Daniel Boone ( University of Arizona, USA) designed . Since the 1970's a variety of auditory sidetone units have been packaged and sold in gradually more minature forms ( i.e. Dr. Ann Dewar's Edinbugh Masker-Scotland, Phonic Ear-DAF, Pacemaster, Thomas Kehoe's Casa Futura System, Dr.George Shames' Vocaltech, Dr.Ronald Webster's Fluency Master ® , Kay Elemetrics Boone-Facilitator and most recently Dr. Joseph Kalinowski's-SpeechEasy ® made by the Janus Development Corporation, North Carolina, USA).
Instrumental Learning and Auditory Sidetone
The use of auditory sidetone lends itself very effectively to a variety of operant behavior modification paradigms in managing stuttering. Behavior modification requires that you identify a specific behavior that you want to eliminate or alter and then carefully and immediately reinforce that behavior. In the case of stuttering you specify the stuttering event ( e.g. a syllable repetition) then you pair it ( e.g. present an auditory response right after a stuttering block) with a buzzer, white noise, or a verbal command. Clinicians have done this for years with electronic lights, toys, or a variety of pre-recorded word signals. This can be performed very quickly (contingent) following the speech"target" behavior.
Clinicians will set up a variety of treatment paradigms that will gradually inhibit or facilitate the desired speech behavior. The intensity or the frequency of the reinforcing signal (auditory sidetone ) can be gradually reduced so that the individual is speaking with his own internal controls learned from many repetitions of the contingent auditory sidetone . When you use delayed auditory feedback as a contingent auditory response to "speech" the speaker learns to change his rate, rhythm,pace, tempo, intonation or loudness to cope with the delay ( his own speech echo). The alteration in speech prosody will often inhibit the stuttering response. Unfortunately this does not carry-over very well because the DAF is not paired to the stuttering specifically but to the speech signal in general. It is therefore difficult to maintain this new speech pattern without the DAF/echo-present. In fact an individual can accommodate to the DAF and loose the fluency evoking new speech pattern after several weeks if the person experiences a negative reinforcement.
Delayed Auditory Sidetone
The effects of speaking in the presence of your own delayed speech signal remains the single most efficient, immediate and initially passive fluency evoking stimili available. This speech-echo-effect is not uniformly facilitated. Some individuals talk slower , some louder, some talk in a slow-monotonous drone, others speak in single word cadence, and still others just can't cope with the echo (i.e. delayed auditory sidetone) without cluttering speech into a jumbled utterance.
For many persons who stutter, delayed auditory feedback of their own speech, especially if received binaurally (two earphones) and at least delayed by 75-90 msec , usually results in slower, easier, controlled intonation and loudness, that automatically reduces their speech hesitations, prolongations, syllable repetitions or hard vocal onset-blocks. There are individual variations of course, and different amounts of effective DAF for each individual should to be expected.
My experience over the years with many of these DAF units [ i.e. Phonic Ear , Kay Elemetrics DAF, Shames/Vocaltech ® , Casa Futura DAF, Fluency Master ® , and SpeechEasy ® ] is that individuals realize almost immediately that DAF works well when it is on, but it does not carry-over consistently without the DAF device. In the past I have encouraged severe PWS to wear these portable binaural DAF units during the day when verbal communication was challenging . I cannot recall any patients I have treated however with DAF or recommended to buy a DAF unit that were able to eventually give up the DAF and sustain a fluent speech pattern without any addiitional significant treatment or psychosocial adjustment.
Fluency Master ®
The introduction of the Fluency Master (FM) in the mid 1990's by Dr. Ronald Webster at the Hollins Communciation Research Institute (Roanoke, Virginia) was a major innovation in the use of auditory-sidetone. It facilitated complete portability and could be used 100% of the speaking day without significant perceptual intrusion. The Fluency Master utilized a "behind-the-ear" hearing aid shell to house the DAF electronics . This was great news for severe chronic secondary stutterers, for whom I believe the Fluency Master was initially designed. Dr.Webster's traditional Precision Fluency Treatment Program continued unmodified when he introduced the FM and continues to this day with excellent fundamental treatment techniques in an intensive two week format. The FM was not intended as a replacement paradigm or a universally applicable technique for all persons who stuttered.
I assessed PWS speech fluency and dispensed the FM at Beaumont Hospital in Royal Oak, Michigan (metro Detroit, USA) because I had a significant group of severe secondary PWS who could not benefit from traditional forms of treatment. To my surprise many individuals who were not severe insisted on trying the FM and purchased it even though they were mild to moderate or that they had acquired in my judgment perfectly adequate fluency controls. To their minds, any real reduction no matter how small ( 1-3%) in stuttering frequency, stress, struggle or improvement in confidence was worth its use.
This remains an important lesson. Persons who stutter, that speak fluently and stutter infrequently do not necessarily resolve their strong anticipatory-anxiety about unseen stuttering. Any reduction in anxiety over stuttering , for some individuals, is worth a great deal.
The Beaumont Stuttering Center dispensed 30 FM devices from the spring of 1992 through the summer of 1994. The FM provided frequency-altered-feedback [FAF] auditory sidetone as well as an undocumented delayed-auditory feeback [DAF]. You could not adjust either the FAF or the DAF. The FM was built into a standard "behind-the-ear" hearing aid shell with a tethered remote microphone that was taped to the PWS mastoid behind their ear. The FAF+DAF feedback signal was delivered through a custom-made earpiece fit into the external auditory canal.
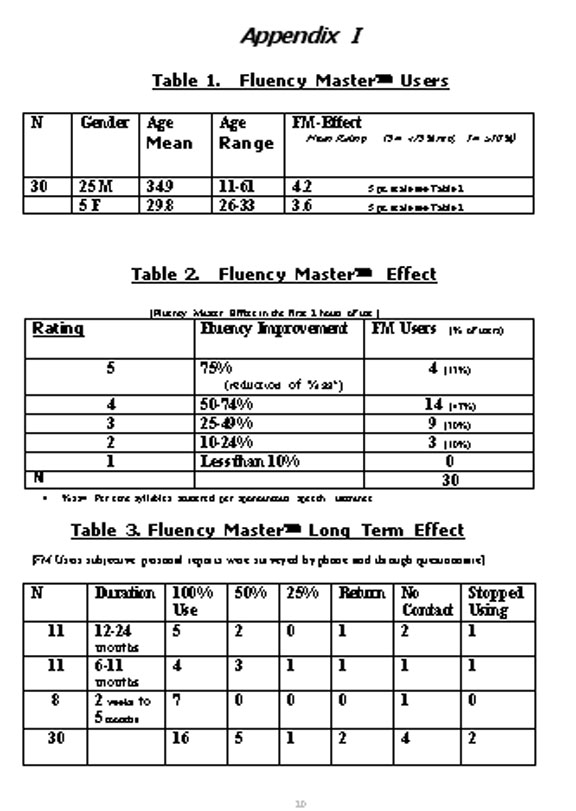
Fluency Master ® Data
In Appendix I , Tables 1-3 I have provided some FM User demographics, data indicating the Immediate Fluency Effects , and data collected indicating some of the Long Term FM Effects of thirty PWS. Table 1 defines the PWS who were fit with the FM devices between 1992 and 1994. There were 30 individuals , 25 males and 5 females, between the ages of 11 and 61 . During the first 2 hours of FM use the males exhibited from 50% to 74% reduction in their stuttering (% syllables stuttered per utterance), and the females exhibited from 25% to 50% reductions in their stuttering. Table 2 defines in more detail the Fluency Master Effect ( i.e. fluency effect in first 2 hours of use) . Examining Table 2 , row one , you can see that 4 FM users exhibited a 75% reduction in stuttering and by including row two, that 18 or 60% of the 30 FM users exhibited 50% or greater reductions in stuttering after only 2 hours of use. Twelve of the thirty FM users (40%) exhibited 24-50% stuttering reductions. Table 3 attempts to illustrate from a subjective (questionnaire) survey how the patients reported their longer term fluency effects. Five of eleven (45%) PWS who had worn the FM for 12 to 24 months reported that they continued to wear the FM 100% of the time with good effects. Two of the eleven reported wearing the FM only 50% of the time with good effects. Sixteen (53%) of the 30 PWS who had worn the FM two weeks to 24 months reported wearing the FM 100% of the time with good effects. Examining column 3 (100% Use) you will notice that 7 of 16 FM users or 44% reported 100% use with good effects in the first 5 months., only 4 of 16 (25%) reported 100% good use from 6 to 11 months and 5 of 16 (31%) reported 100% good effect after one to two years. There appears to be a "loss of effect " for a number of users. Conversely , I can also report that I know of one of these FM users who has maintained 100% use with good speech fluency effects for over ten years .
SpeechEasy ®
The SpeechEasy ® was developed in the past three years by a team of speech pathologists and audiologists from East Carolina University ( Greenville, North Carolina,USA) under the principle direction of Dr.Joseph Kalinowski. Dr. Kalinowksi was a colleague of Dr.Ronald Webster's and at one time, I believe he wore a FM as he is a PWS. Dr.Kalinowski has conducted and published a number of peer-reviewed scientific articles on auditory sidetone especially the effects of unilateral delayed auditory and frequency-altered feedback. The SpeechEasy ® (SE) a product of the Janus Development Company of Greenville, North Carolina is a completely digital device that can be specifically programmed through companion software to custom set the DAF or FAF signal that evokes the most stuttering reduction in each individual. The SE is far less conspicuous than the FM and can be custom fit to be inserted into the external auditory canal. Like the FM it is only monaural (i.e. worn in one ear) and provides less consistent effects than binaural devices.
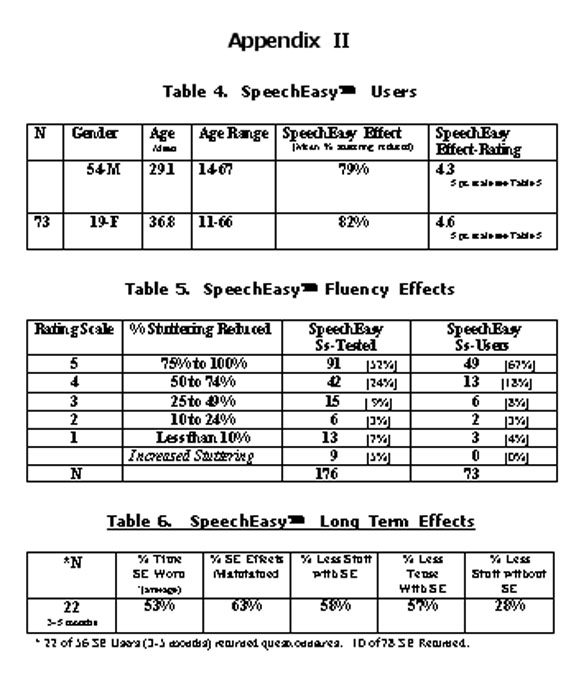
SpeechEasy ® Data
In Appendix II ,Tables 4-6 I have provided some SE User demographics ,some immediate SpeechEasy Fluency Effects and some subjective ( questionnaire survey) long term SE Fluency Effects. Table 4 briefly describes the seventy three SE Users that chose to purchase the SE after an evaluation at the Beaumont Stuttering Center. Fifty-four were males between the ages of 14 years and 67 years ( mean of 29.1) and 19 were females between the ages of 11 years and 66 years of age ( mean of 36.8). Column five of Table 4 indicates that the average reduction in stuttering ( stuttering=% syllables stuttered) after wearing the SE for at least one hour (immediate effect) was 79% for the males and 82% for the females. In Table 5, I describe the immediate fluency effect ( % stuttering reduced) in 176 PWS who were evaluated for the SE. In column three of Table 5 you will notice that 91 of the 176 (52%) PWS who were evaluated for the SE had a 75% to 100% immediate fluency effect (reduction in stuttering). In column 4 of Table 5 , 49 of the 73 (67%) PWS who decided to purchase the SE had a 75% to 100% immediate fluency effect. It is interesting to observe that eleven individuals who decided to purchase the SE had a 50% or less reduction in stuttering. Further, 9 of the 176 (5%) PWS who were evaluated for the SE experienced an increase in their stuttering as an immediate effect.
Longer term effects have only been evaluated subjectively by a questionnaire survey. Table 6 illustrates that 22 of 56 SE users, of 3 to 5 months duration , have returned their survey to indicate that on average (1) they wear their SE 53% of the time, (2) 63% of the immediate fluency effect remains, (3) they stutter 53% less when wearing the SE, (4) they are 57% less tense when wearing the SE, and (5) they stutter 28% less without the SE.
Summary: It is clear that the fluency effects of the SpeechEasy and Fluency Master are not simple or uniform. Further , the data presented is empirical and not scientifically tested. I hope to bring a substantial number of the SE Users back into the clinic to document more objectively their fluency effects after 12-18 months of use. Many more evidenced-based empirical and scientifically controlled studies are needed. Auditory sidetone remains a viable and important clinical tool in the total management of stuttering.
Caveats for: Speech-Language Pathologists and Persons Who Stutter.
- Auditory sidetone continues to be a valuable clinical adjunct to a total treatment program for an important number of persons-who-stutter.
- Electronic devices without speech pathology treatment before,during and/or after their use are short-circuited.
- If auditory sidetone is effective in evoking fluency it must be custom-fit to each individual and their total treatment program.
- We cannot yet predict or adequately describe the type of PWS who would be best suited for auditory sidetone.
- Traditional treatment remains at the forefront of clinical choice.
Scientific Investigations on the Effects of Auditory Sidetone on Stuttering
Selected References Richard M.Merson,Ph.D.
William Beaumont Hospital
Royal Oak, Michigan
1. Black, J.W. "The Effects of Delayed Sidetone Upon Vocal Rate and Intensity". Journal of Speech and Hearing Disorders (XVI) Pp.56-60, 1951.
2. Cherry, C.,Sayers,B. "Experiemnts on the total inhibition of stammering by external control and clinical results." JOURNAL OF PSYCHOSOMATIC RESEARCH, 910 Pp.233-246, 1956.
3. Sutton, S, Chase, R.A. " White Noise and Stuttering." JOURNAL OF SPEECH HEARING RESEARCH (4), Pp.72, 1961.
4. Fransella, F., Beech,H.R. "An Experimental analysis of the effect of rhythm on the speech of stutterers." BEHAVIOR RESEARCH THERAPY, (3) Pp.195-201, 1965.
5. Curlee, R., Perkins, W. "Conversational rate control therapy for stuttering." JOURNAL OF SPEECH HEARING DISORDERS, (34) Pp.245- 250, 1969.
6. Wingate,M.R. "Effect on Stuttering of changes in audition". JOURNAL OF SPEECH AND HEARING RESEARCH, (13), Pp.861-873, 1970.
7. Van Riper,Charles. The Nature of Stuttering. Chapter 14, Pp. 382-403. Prentice-Hall Inc. Englewood Cliffs, N.J. 1971
8. Ryan, B , VanKirk, B., "The Establishment, Transfer and Maintenance of Fluent Speech in 50 Stutterers using Delayed Auditory Feeback and Operant Procedures." JOURNAL OF SPEECH AND HEARING RESEARCH, (39) , 1974.
9. Burke,B.D. "Susceptibility to delayed auditory feedback and dependence on auditory or oral sensory feedback." JOURNAL OF COMMUNICATION DISORDER. (8:1), Pp.75-96, 1975.
10. Burke, B.D., "Variables affecting stutterer's initial reactions to delayed auditory feedback." JOURNAL OF COMMUNICATION DISORDER, June (8:2), Pp. 141-155, 1975
11. Brady, J.P., Berson, J. "Stuttering, dichotic listening and cerebral dominance." ARCHIVES GENERAL PSYCHIATRY, November (32:11), pp. 1449-1452, 1975.
12. Yairi,E. "Effects of Binaural and Monaural Noise on Stuttering". JOURNAL OF AUDITORY RESEARCH (16) Pp. 114-119, 1976.
13. Timmons, B.A., Boudreau,J.P. "Delayed auditory feedback and the speech of stuttering and non-stuttering children." PERCEPTUAL MOTOR SKILLS , April (46:2) Pp.551-555, 1978.
14. Martin, R., Haroldson,S.K. "Effects of five experimental treatments of stuttering".JOURNAL OF SPEECH HEARING RESEARCH ,March (22:1) Pp.132-146, 1979.
15. Webster, R.L.,Dorman,M.F. "Decreases in Stuttering Frequency as a function of continuous and contingent forms of auditory masking". JOURNAL OF SPEECH AND HEARING RESEARCH,(13) Pp.82-86, 1979.
16. Dewar, Ann, A.D.Dewar, W.T.S.Austin and H.M.Brash." The Long Term Use of an Automatically Triggered Auditory Feedback Masking Device in the Treatment of Stammiering"" BRITISH JOURNAL OF DISORDERS OF COMMUNICATION,( vol.14, no.3) 1979.
17. Stephen, S.C., Haggard, M.P. "Acoustic properties of masking/delayed feedback in the fluency of stutterers and controls." JOURNAL OF SPEECH HEARING RESEARCH,September (23:3), pp. 527-538, 1980.
18. Martin,R. G. Siegel, L. Johnson, and S. Haroldson, "Sidetone Amplification,Noise and Stuttering." JOURNAL OF SPEECH AND HEARING RESEARCH, (27) Pp.518-527, 1984.
19. Fukawa, T., Yoshida,S. "Sex difference in susceptibility to delayed auditory feedback in oral rading tasks." SHINRIGAKU KENKYU, August, (59:3), Pp.144-150, 1988.
20. Fukawa,T. Yoshioka,H. Ozawa,E., Yoshida, S. "Difference in Susceptibility to delayed auditory feedback between stutterers and nonstutterers. JOURNAL SPEECH HEARING RESEARCH ,September (31:3), Pp. 475-479, 1988.
21. Harrington, J. "Stuttering, delayed auditory feedback and linguistic rhythm." JOURNAL OF SPEECH AND HEARING RESEARCH, (31) Pp.36-47, 1988.
22. Kalinowski, J.S., Armson, J., Roland-Mieszkowski, M.,Stuart,A., Gracco,V.L."Effects of alterations in auditory feedback and speech rate on stuttering frequency. LANGUAGE AND SPEECH, (36), Pp.1-16, 1991.
23. Ryan,B.P., Van Kirk, R.B. "Programmed stuttering treatment for children:comparison of two establishment programs through transfer, maintenance, and follow-up." JOURNAL OF SPEECH HEARING RESEARCH, February (38:1) Pp. 61-75, 1995.
24. Kalinowski,J. Stuart,A. ® Stuttering amelioration at various auditory feedback delays and speech rates." EUROPEAN JOURNAL DISORDERS COMMUNICATION, (31:3) Pp.259-269, 1996.
25. Stuart, A. Kalinowski, J. Rasttter,M.P. " Effect of monaural and binaural altered auditory feedback on stuttering frequency." JOURNAL ACOUSTICAL SOCIETY OF AMERICA. June (101:6) Pp.3806-3809, 1997.
26. Ingham,R.J., Moglia,R.A.,Frank,P., Ingham, J.C., Cordes, A.K. "Experimental investigation of the effects of frequency-altered auditory feedback on the speech of adults who stutter." JOURNAL SPEECH LANGUAGE HEARING RESEARCH, April, (40:2), Pp.361-372, 1997.
27. Natke, U. "Reduction of stuttering frequency using frequency-shifted and delayed auditory feedback". FOLIA PHONIATRICA LOGOPEDICS.July-August (52:4) Pp. 151-159, 2000.
28. Ingham, R.J. Sato,W., Finn,P., Belknap,H. "The modification of speech naturalness during rhythmic stimulation treatment of stuttering." JOURNAL SPEECH LANGUAGE HEARING RESEARCH. August, (44:4) Pp.841-852, 2001.
29. Stuart, A., Kalinowski, J,Rastatter,M.P., Lynch,K. "Effect of delayed auditory feedback on normal speakers at two speech rates." JOURNAL ACOUSTICAL SOCIETY AMERICA. May, (111:5) Pp. 2237-2241, 2002.
Some Electronic DAF devices:
Facilitator, Daniel Boone, Ph.D. Kay Elemetrics Corp. Lincoln Park, New Jersey, USA. www.kayelemetrics.com
Fluency Master, National Association for Speech Fluency,228 Birch Drive New Hyde Park, NY 11040-2322. www.stutteringcontrol.com
SpeechEasy, Joseph Kalinowski, Ph.D., Janus Development Corp. Greenville, North Carolina. www.speecheasy.com
CasaFutura DAF, Thomas Kehoe, CasaFutura Tech. Co. www.casafuturatech.com
September 17, 2003